Surgical system
A surgical operation and tracking system technology, applied in the field of end effectors, can solve the problems of entering patients, saw blades limiting cutting accuracy, etc.
- Summary
- Abstract
- Description
- Claims
- Application Information
AI Technical Summary
Problems solved by technology
Method used
Image

Examples
Embodiment Construction
[0030] The inventive concept will now be described more fully hereinafter with reference to the accompanying drawings, in which examples of embodiments of the inventive concept are shown. The inventive concepts may be embodied in many different forms and should not be construed as limited to the embodiments set forth herein. Rather, these embodiments are provided so that this disclosure will be thorough and complete, and will fully convey the scope of the various inventive concepts to those skilled in the art. It should also be noted that these embodiments are not mutually exclusive. Components in one embodiment may be defaulted to be present in, or used in, another embodiment.
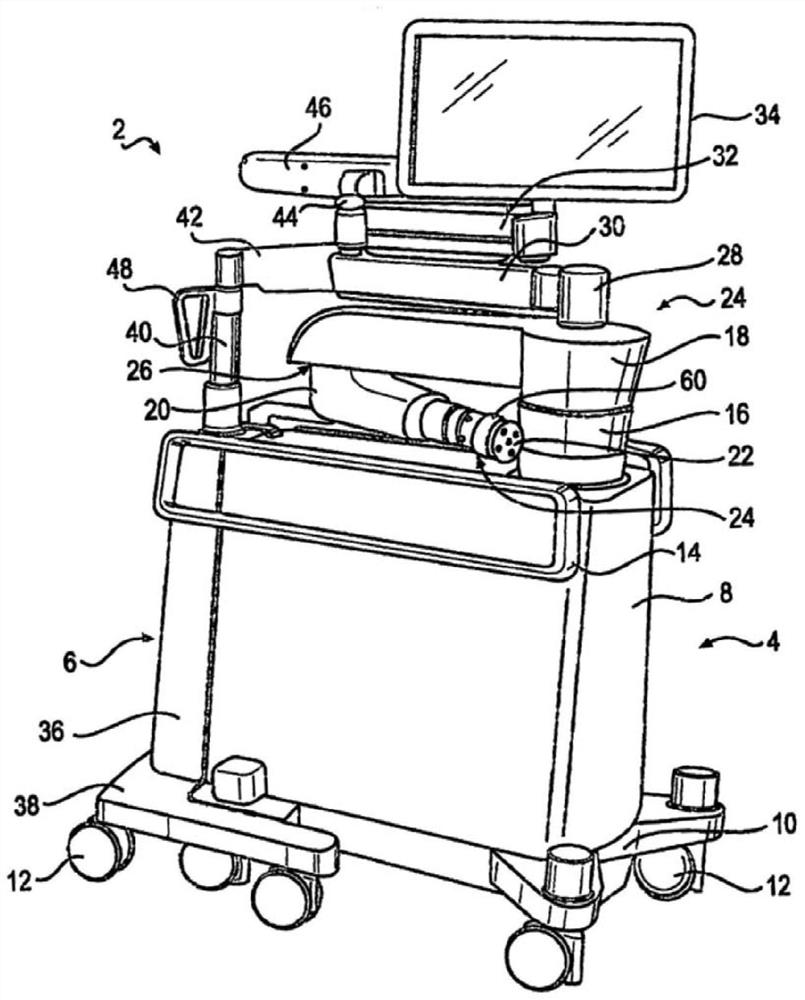
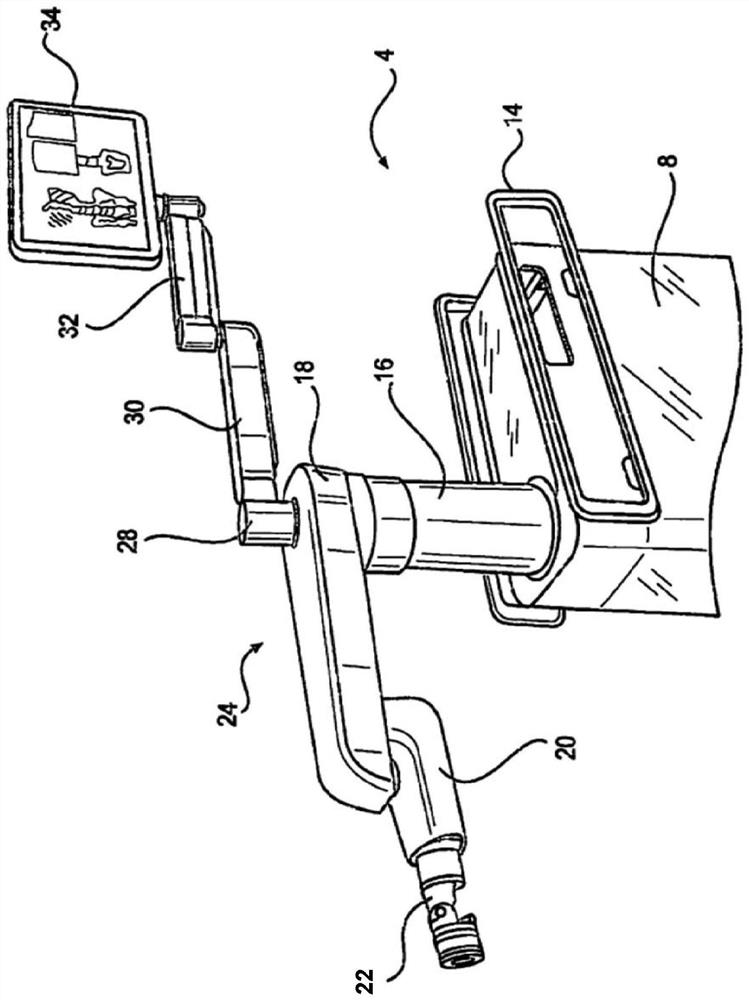
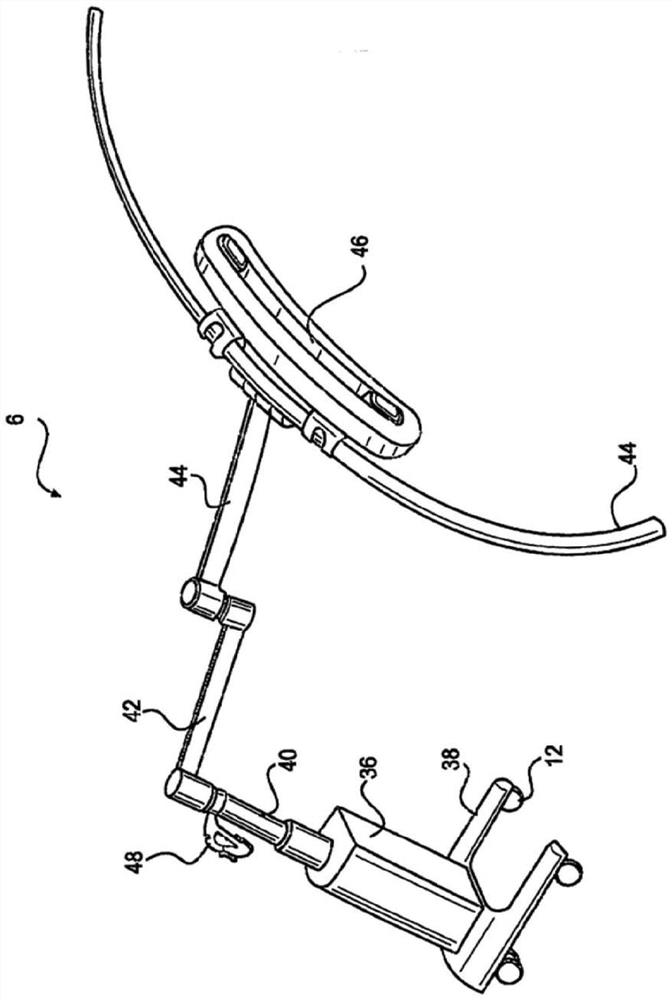
[0031] Various embodiments disclosed herein relate to improvements in the operation of surgical systems when performing surgical interventions requiring osteotomies. A passive end effector connectable to a robotic arm positioned by a surgical robot is disclosed. Passive end effectors have a pair of...
PUM
 Login to View More
Login to View More Abstract
Description
Claims
Application Information
 Login to View More
Login to View More