The rising cost of health care is unsustainable.
This suggests some substantial communication problems within the subsystem navigated by PCMH.
A lack of
clarity on the respective roles of PCP's and specialists undoubtedly may contribute to coordination issues among specialists and PCP's.
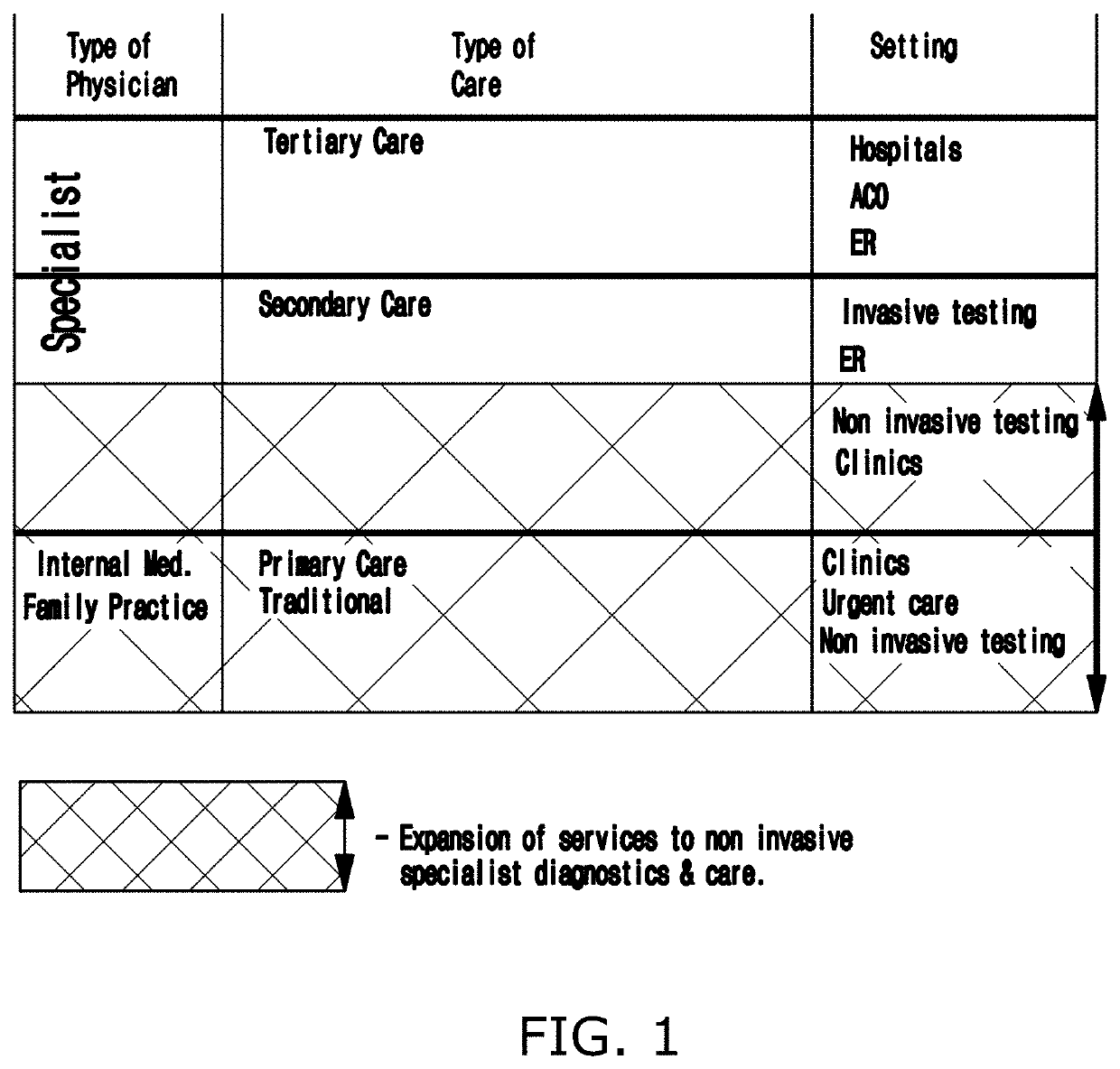
Thus, significant fragmentation of care exists for patients with any chronic conditions, especially for patients with multiple chronic conditions.
Moreover, shrinking access to specialists within each insurance network leaves significant gaps and creates barriers to care delivery even with the best primary care coordination.
The shortage of primary care physicians makes it more difficult for
special populations, like full-time employees or patients with multiple chronic conditions, to access primary, secondary or
tertiary services.
The traditional fee-for-
service system lacks efficiency and causes a lot of
frustration not only to patients but also to practicing physicians.
Further compounding the problem, the shortage of primary care physicians makes it more difficult for
special populations, like full-time employees or patients with multiple chronic conditions, to access primary or secondary preventive services.
The cost of care for patients with chronic conditions is higher than the general
population with differences in quality of care
stemming from gender and racial differences.
Patients with chronic conditions spend more for healthcare and experience more hardship with paying medical bills while physicians taking care of patients with chronic conditions believe that the needs of these patients are not being met and physicians report difficulties in coordinating care of patients with chronic conditions.
Although specialist care is cited as being at least 10 times more expensive in the US than primary care, the only attempts at decreasing such costs have been through employing a “gate keeping” strategy to primary care, which ultimately results in more inefficiency and greater distrust among patients.
Thus, significant fragmentation of care delivery exists for patients with any chronic conditions, and patients with multiple chronic conditions, who represent 50-70% of the general
population, are forced to see three to four different doctors each at different offices.
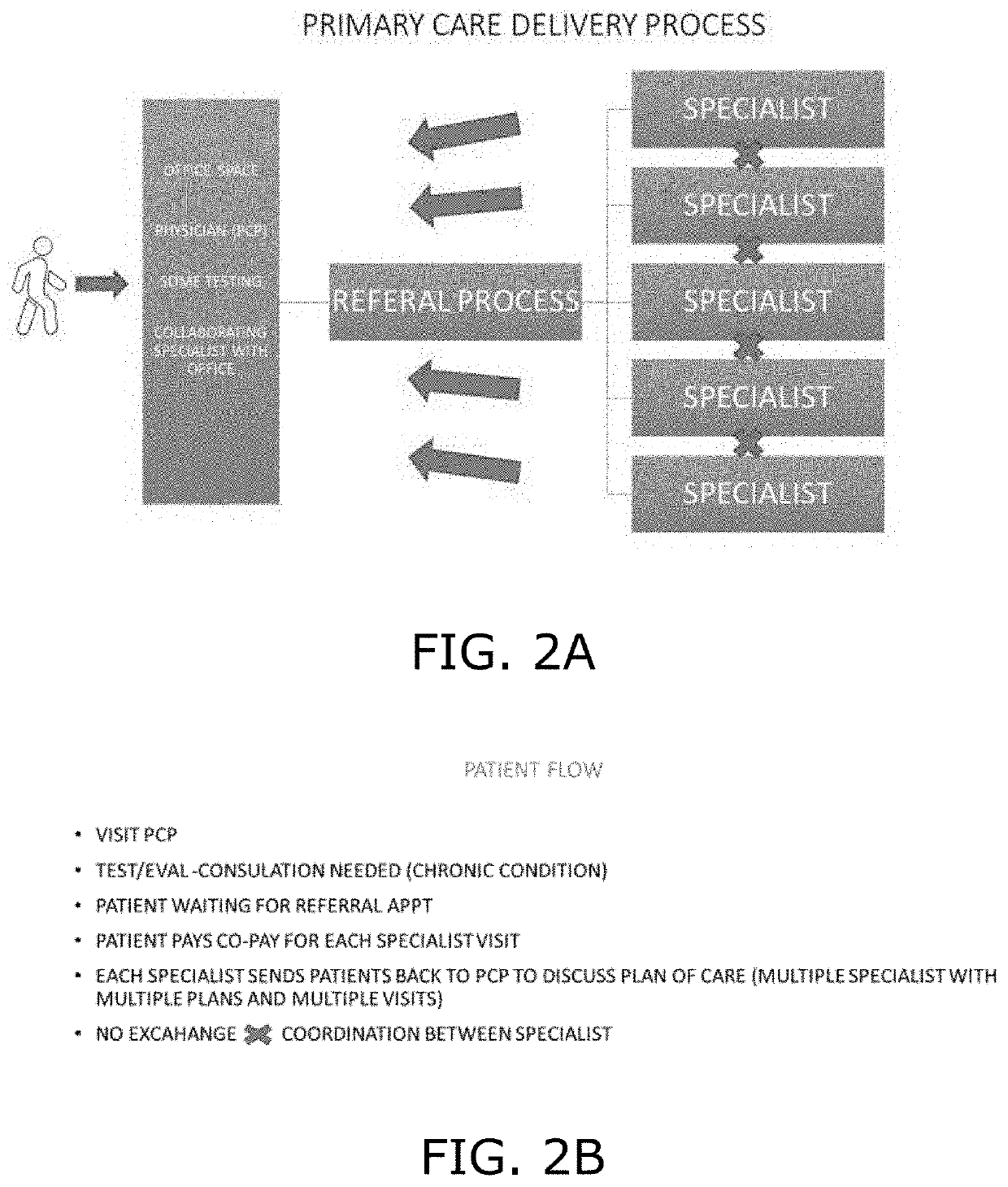
In short, when primary care physicians coordinate advanced care and send referrals to specialists to secure secondary preventive services the already fragmented healthcare delivery process is made even more inefficient and fragmented for patients, especially those with chronic conditions.
Furthermore, US National Center for Health Statistics describes chronic diseases as illnesses that generally cannot be prevented by vaccines or cured by medication, nor do they just disappear.
Many barriers to care delivery are inherent in this model and include, for example,
limited access to specialist, lack of coordination between multiple specialist and
increased risk for medical errors due to multiple plans of care presented to the patients by each specialist and PCP.
The diagnosis of chronic conditions, especially multiple chronic conditions, carries very significant increase in cost of care delivery.
These scores are not used in the
primary care physician offices since they cannot be applied to direct care delivery, for instance, they cannot be applied to instruct which medication should be used to treat the symptoms and prevent worsening of diseases.



 Login to View More
Login to View More  Login to View More
Login to View More