Flexible four-finger rehabilitation robot capable of being driven remotely
A rehabilitation robot and remote technology, applied in the direction of passive exercise equipment, physical therapy, etc., can solve the problems of inability to exchange left and right hands, inability to adjust the length, uncomfortable wearing, etc., to achieve improved safety, simple and convenient control, and wearable comfortable effect
- Summary
- Abstract
- Description
- Claims
- Application Information
AI Technical Summary
Problems solved by technology
Method used
Image


Examples
Embodiment Construction
[0027] The present invention is described in further detail now in conjunction with accompanying drawing. These drawings are all simplified schematic diagrams, which only illustrate the basic structure of the present invention in a schematic manner, so they only show the configurations related to the present invention.
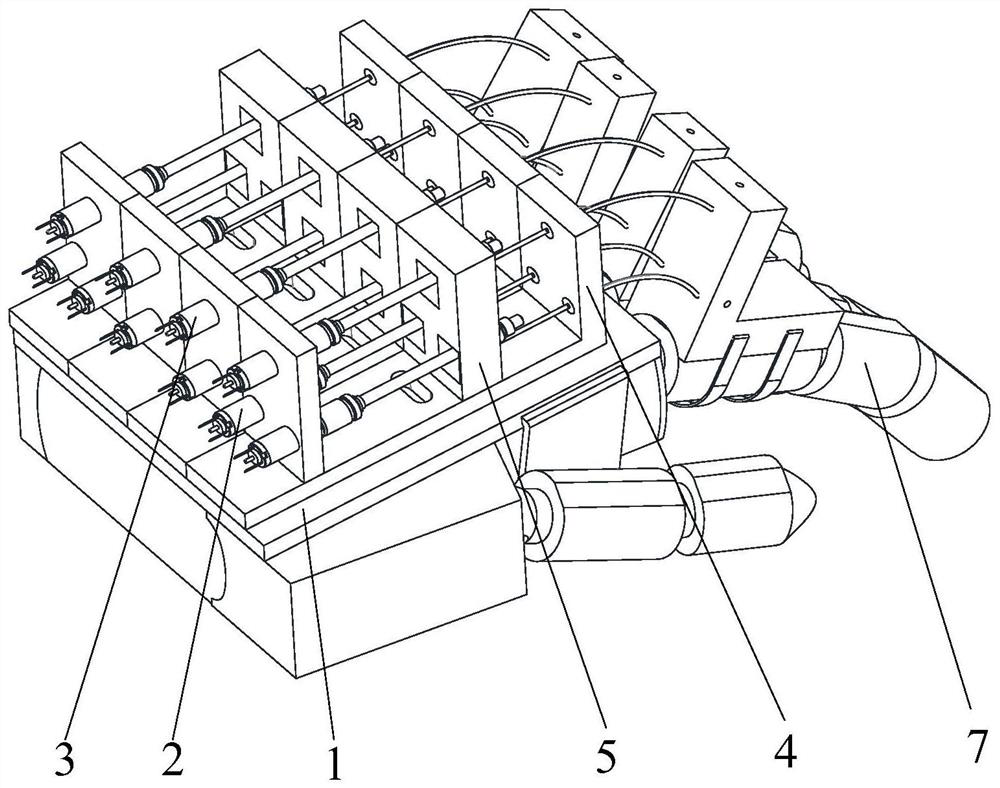
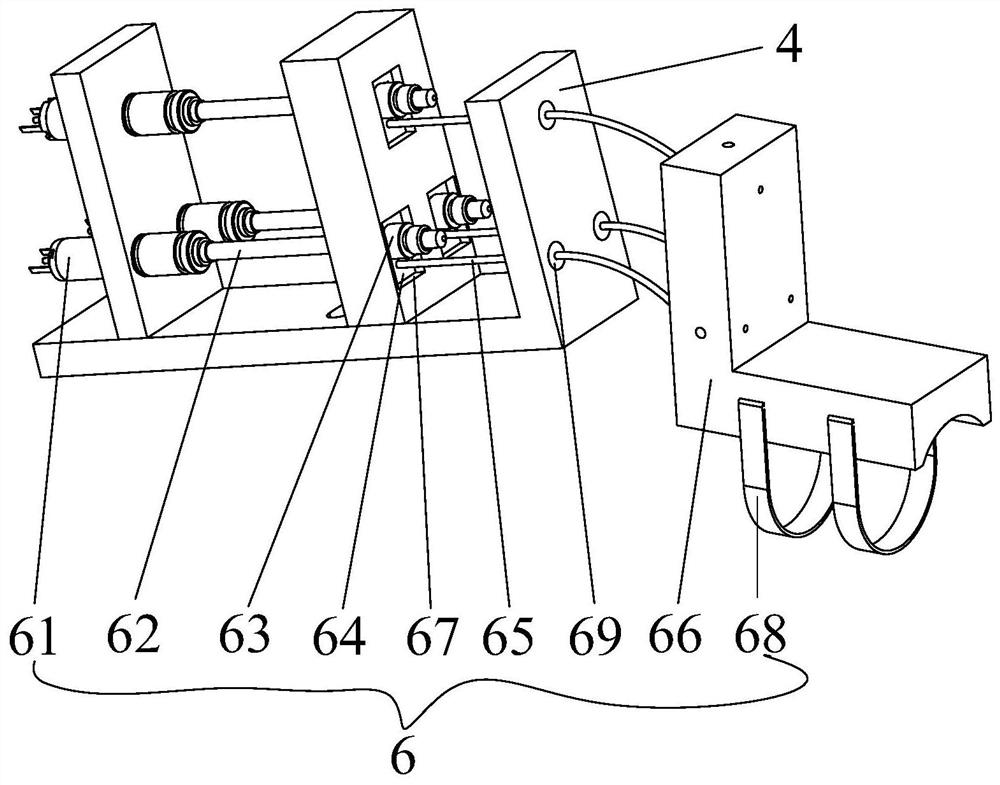
[0028] In the description of the embodiment of the present invention, it needs to be stated that: when the finger rehabilitation robot is worn on the human hand, the direction where the finger points is forward, the direction where the palm is located is the back, the side where the little finger is located is left, and the side where the thumb is located is right , the back side of the palm is the upper side, and the palm side is the lower side, the embodiment of the present invention Figure 1-Figure 7 The hand model 7 is used to replace the patient's hand.
[0029] like Figure 1-Figure 7 The shown specific embodiment of a flexible four-finger rehabilitat...
PUM
 Login to View More
Login to View More Abstract
Description
Claims
Application Information
 Login to View More
Login to View More