Traditional medical and surgical treatment of patients with failing pump function of the heart is limited to blood-contacting devices which are technically difficult to install and result in complications related to such blood contact as well as technical aspects of device installation.
Inadequate cardiac output remains a cause of millions of deaths annually in the United States.
However, all currently available devices require too much time to implant to be of value in acute resuscitation situations, resulting in loss of life before adequate circulatory support can be provided.
Furthermore, other non-blood contacting devices similar to the current invention provide inadequate augmentation of cardiac function.
DCC devices have been shown to only benefit hearts with substantial degrees of LV failure.
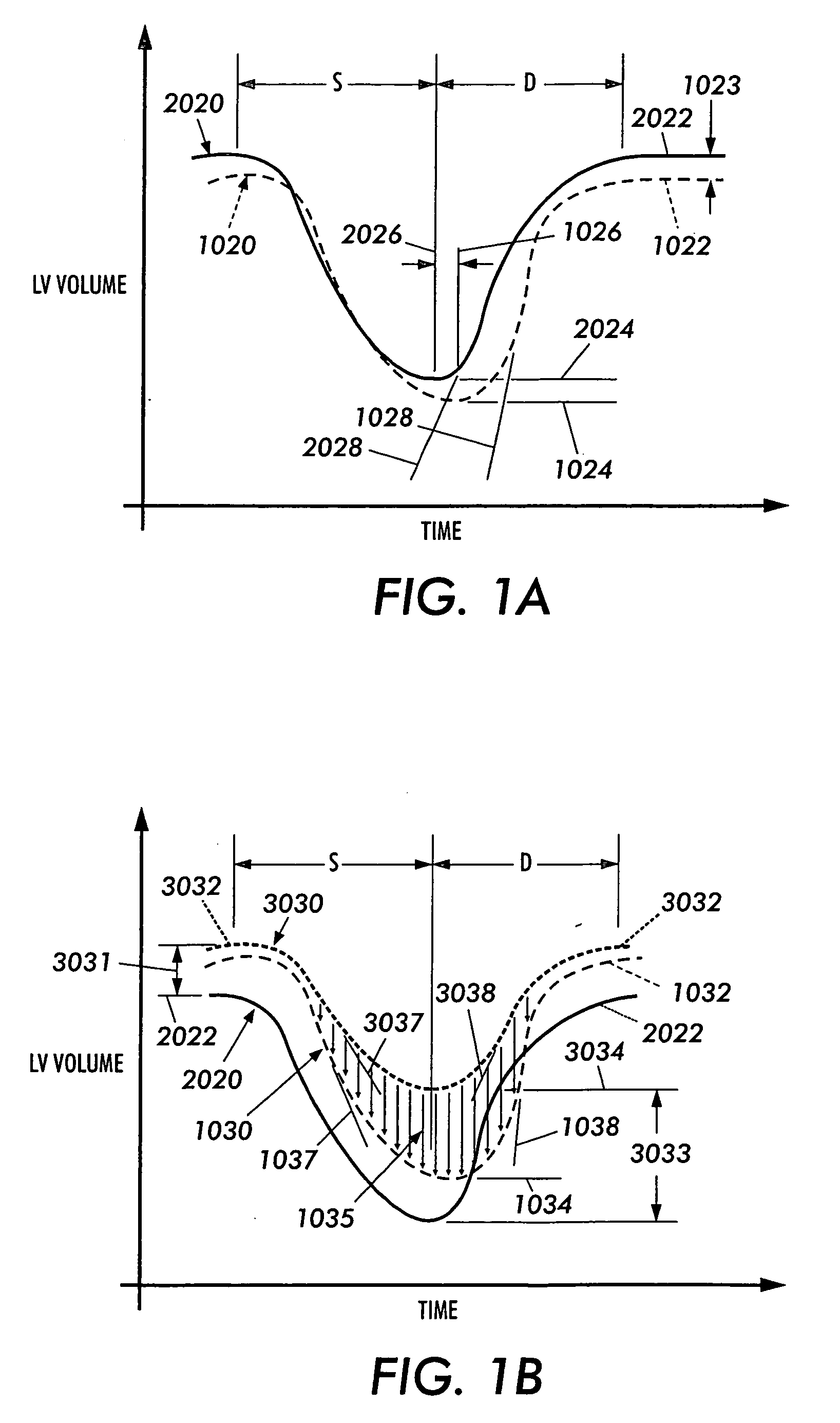
Specifically, DCC techniques only substantially improve the systolic function of hearts in moderate to severe heart failure.
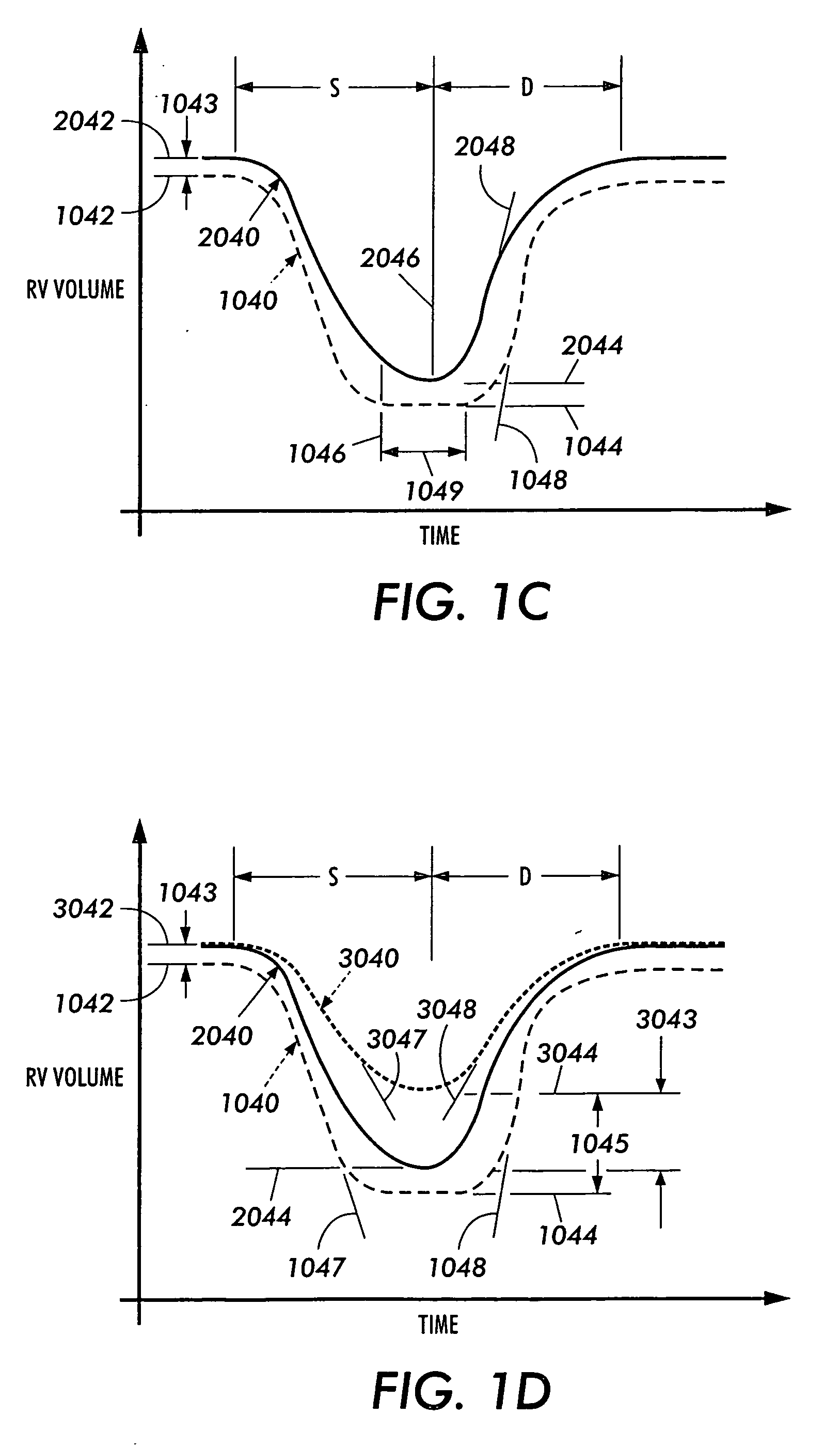
DCC techniques clearly have a negative effect on diastolic function (both RV and LV diastolic function).
This is exhibited by reductions in diastolic volume that, in part, explains DCC's inability to effectively augment the heart without at least moderate degrees of failure.
This also explains DCC's efficacy being limited to sufficient degrees of LV size and / or dilatation, with significant dependence on preload, and / or ventricular filling pressures.
In addition, DCC devices have negative effects on the dynamics of diastolic relaxation and, in effect, reduce the rate of diastolic pressure decay (negative dP / dt max), increasing the time required for ventricular relaxation.
First, and foremost, these techniques do not provide any means to augment diastolic function of the heart necessary to overcome their inherent drawback of “effectively” increasing ventricular stiffness.
Clearly, RV diastolic function is impaired to a far greater degree by DCC due to the nature both the RV wall and intra-cavity pressures.
Furthermore, studies of DCC devices have all overlooked the relevant and dependent impact these techniques have on right ventricular dynamics, septal motion and overall cardiac function.
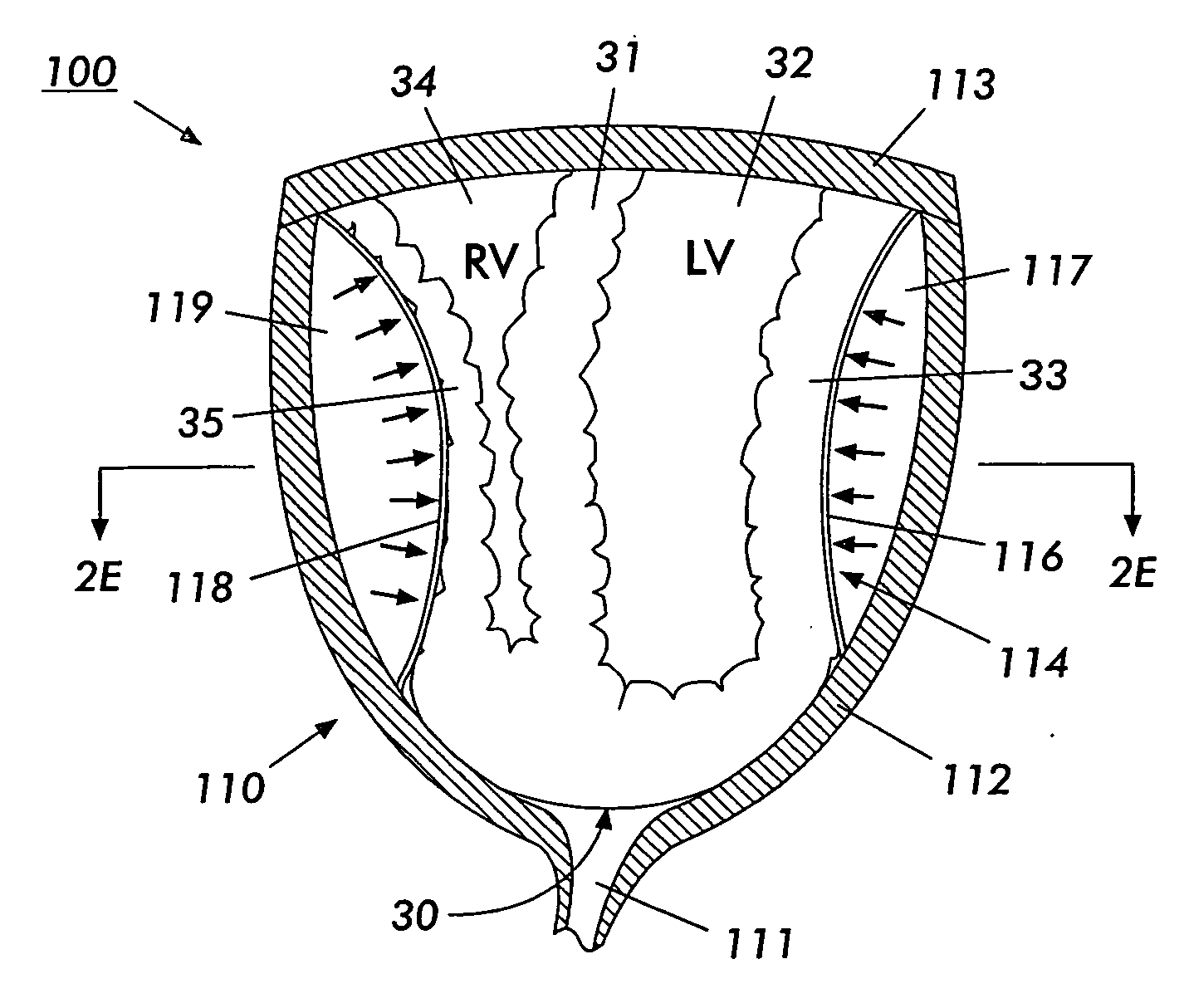
Because the right ventricle is responsible for providing the “priming” blood flow to the left ventricle, compromising right ventricular function has a necessary secondary and negative impact on left ventricular pumping function when these load-dependent devices are utilized.
Another related and fundamental drawback to DCC devices is their inability to continuously monitor ventricular wall motion and chamber dynamics that are intuitively critical to optimizing the assist provided by such mechanical actions on the right and left ventricular chambers which behave in an complex, inter-related fashion.
Finally, studies regarding DCC methods have failed to adequately examine the effects of these devices on myocardial integrity.
These factors make it difficult to pre-operatively define the optimum liner time-displacement profiles or hydraulic drive unit control parameters capable of satisfying every patient's unique DMVA requirements.
It is well known that diseased heart tissue can be very fragile, i.e. such tissue is of lower resistance to shear forces and / or less tensile strength than healthy heart tissue.
Thus physicians lacking due caution can easily perforate or injure diseased hearts with their fingers while applying gentle pressure during open heart massage by the high pressure at a finger tip adjacent to a low pressure or pressure void between fingers.
However, the persistent application of forces to the heart can also cause potentially catastrophic damage to the heart by fatiguing and severely bruising the heart muscle and / or abrading the heart surface, which can ultimately prevent the heart from functioning.
This is essential, given that any such DCC device that encompass the ventricles and applies external forces will have inherently negative impacts on diastolic function.
Inadequate size and / or diastolic assist will predominantly compromise RV filling, resulting in diminished RV output, and in turn, reductions in overall cardiac output.
Functional interactions between the right ventricle and left ventricle under mechanical systolic and diastolic actuation are relatively complex and difficult to describe and / or characterize.



 Login to View More
Login to View More  Login to View More
Login to View More