Recent trends suggest that the United States (and to a lesser extent, other industrialized nations throughout the world) are facing a looming
public health crisis, the byproduct of an aging
population and the increasingly
poor nutrition and fitness regimens of the populace.
This has led to a dramatic upswing in
obesity-related
disease states, including
Type II diabetes, cardiovascular
disease, and hypertension, with
treatment costs associated with these
disease states estimated at $117 billion, and is exerting tremendous upward pressure on healthcare costs in the US, which are currently forecast to reach 16% of GDP by 2006.
This trend, which is clearly unsustainable, has led to a slow but deliberate shift in the orientation and focus of the traditional healthcare
delivery system, as payers and practitioners alike seek more effective and efficient alternatives to traditional
disease treatment programs, such as disease
state management and prevention.
While the market for
consumer-oriented health and wellness products and services is large and growing, research consistently demonstrates that the majority of such offerings (be they diet programs or health club memberships) fail to deliver the sort of measurable, sustainable results that would warrant their expense.
Furthermore, while recent advances in technology (in particular, the emergence of
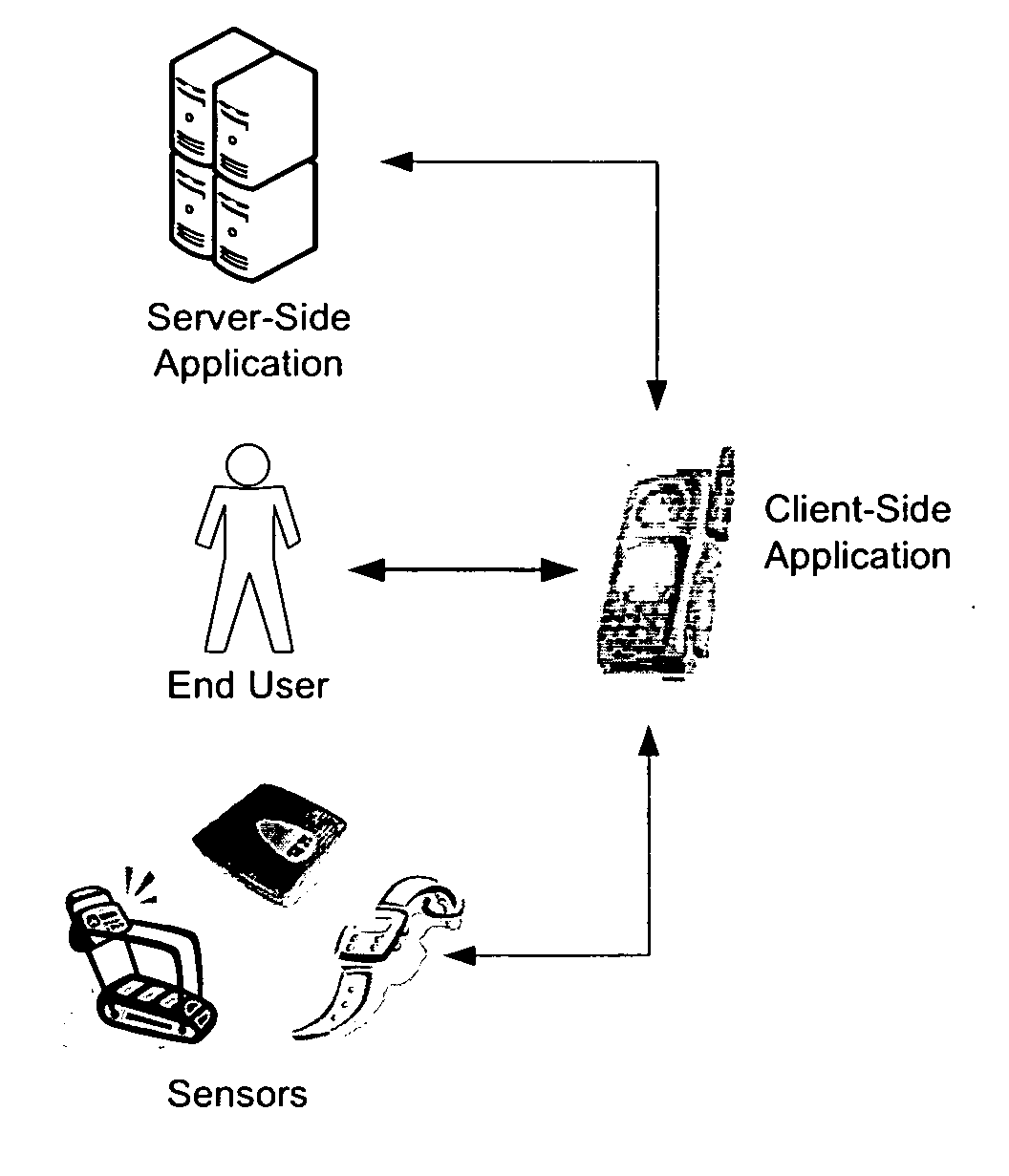
wireless, Internet-enabled mobile devices) has led to a broad array of technology-based solutions, each aimed at improving the health and wellness of an individual, a review of the prior art suggests that these solutions each have one or more disadvantages that may ultimately limit their effectiveness—to wit: Not optimally integrating (and balancing) the roles of practitioners and end users.
Practitioner-driven solutions (such as wireless health monitoring solutions) often treat the
end user as little more than a passive instruction follower, while
consumer-driven solutions provide little in the way of coaching and guidance, often requiring the
end user to act as their own practitioner or to access / integrate practitioner knowledge in an awkward fashion, limiting their usefulness.
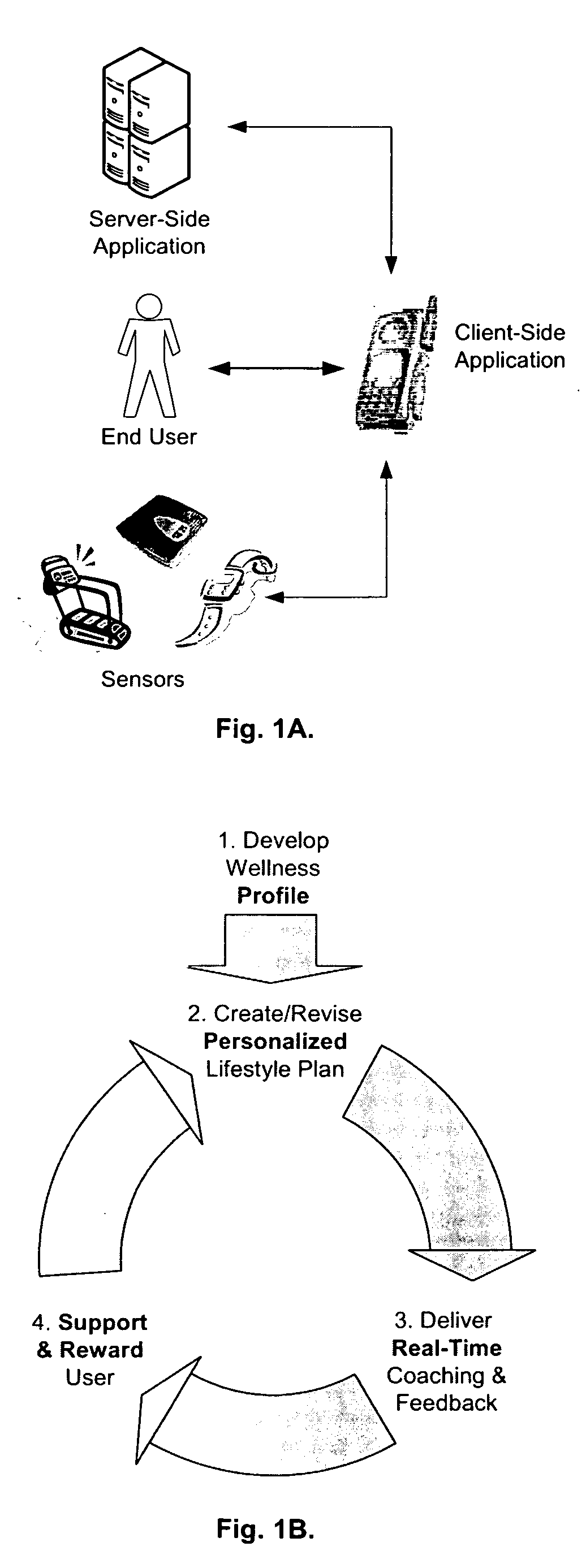
Lacking the ability to address all of the “enablers” of health and wellness, including (but not limited to) diet, exercise, medication and vital sign testing.
Such single-point solutions (e.g. mobile exercise
instructional software) require the user to either ignore the other enablers, or to employ multiple solutions to address all of the enablers, again limiting their usefulness.
Such solutions (such as diet tracking
software packages) assume that the
user needs little motivation to comply with their specified plan, which conflicts with published research highlighting the need for behavioral modification.
However, the referenced design is highly practitioner-driven, encompasses only selected enablers of health and wellness, and does not focus on the driver of plan compliance.
The teaching, however, focuses primarily on the nutritional and
dietary requirements and activity of the
end user, is not configured to allow practitioner generation of integrated lifestyle plans, nor does it incorporate functionality intended to drive plan compliance, such as rewards or the ability to share plans and results with a broader
community.



 Login to View More
Login to View More  Login to View More
Login to View More