Current monitors fall into two classes, namely activity monitors and inertial monitors, both of which have disadvantages and limitations that make them incapable of continuous monitoring of movement disorders in
ambulatory settings.
These monitors are usually small, unobtrusive devices resembling watches or brooches which are worn by the subject for long periods of time such as days or weeks outside of the clinical setting.
While they are useful for recording the gross activity levels of the subject, and they may be comfortable and unobtrusive enough to be worn by the subject for longs periods of time, they are only useful in measuring non-subtle symptoms of movement disorders such as activity versus rest cycles.
These devices, also known as actigraphers, typically measure movement counts per minute which make even simple determinations such as determining the wake-up time challenging.
Consequently, actigraphers are inappropriate for continuous
ambulatory monitoring of movement disorders such as in Parkinson's
disease.
These devices are useful for measuring all symptoms of movement disorders, but because of their larger, obtrusive size and short operational times, are not useful for measuring symptoms outside of
clinical settings or for long periods of time.
Additionally, current movement disorder monitoring devices also lack aiding sensors, such as absolute measures of position.
Movement monitoring devices and systems that overcome challenges of physical size,
power consumption, and
wireless synchronization are currently unavailable and have significant potential in numerous applications including clinical practice and research.
Current methods of
motor system assessment for PD are inadequate because they are intermittent, subjective, and have poor sensitivity.
The UPDRS and other clinical rating scales are coarse, subjective, momentary, stressful to the patient, and insensitive to subtle changes in the patient's motor state.
The value of these scales is limited because each patient's motor state varies continuously throughout the day and can be altered by diet, activity, stress, quality of sleep, or
anxiety.
In particular, dyskinesias are often at their worst during normal daily activities and may have a diurnal pattern.
Medical devices that have been designed to more precisely and objectively measure the
motor symptoms also have this limitation.
Patient diaries and other methods of self reporting are sometimes used to determine patients' motor condition throughout the day, but these are often inaccurate, incomplete, cumbersome, and difficult to interpret.
These methods are also susceptible to selection, perceptual, and recall bias.
Patients generally have poor consistency and validity at assessing the clinical severity of their impairment.
Patients with mild or moderate
dyskinesia may be unaware of their impairment and may have poor recall.
However, these systems are expensive, can only measure movements in a restricted laboratory space, and cannot be used to observe patients at home.
These systems are not practical for home settings.
The
system can operate continuously and wirelessly
stream data via
Bluetooth to a
laptop for over 3 h at distances up to 100 m. However the system is too cumbersome and difficult to use in a home study due to the wires connecting the sensors and central recording unit, the battery life is too short, and the interconnecting wires may be hazardous during normal daily activities.
However, typical activity monitors cannot distinguish between
motor activity caused by voluntary movement, tremor, or
dyskinesia.
They do not have sufficient bandwidth, memory, or sensors for precise monitoring of motor impairment in PD.
They also cannot distinguish between periods of hypokinesia and naps.
This devices can
record data continuously and store it on an on-board memory for up to 12 h. However, 1) the due to their size it is difficult for several of these devices to be used at the same time (e.g.
wrist,
ankle, waits,
trunk), 2) the storage capability is limited to a single day and consequently it is difficult to conduct multiple day studies, and 3) the devices are not synchronized.
Movement monitoring devices and systems that overcome the challenges of 1) physical size (volume), 2)
power consumption, 3)
wireless synchronization, 4)
wireless connectivity, 5) automatic calibration, and 6)
noise floor; are currently unavailable and have significant potential in numerous applications including clinical practice and research.
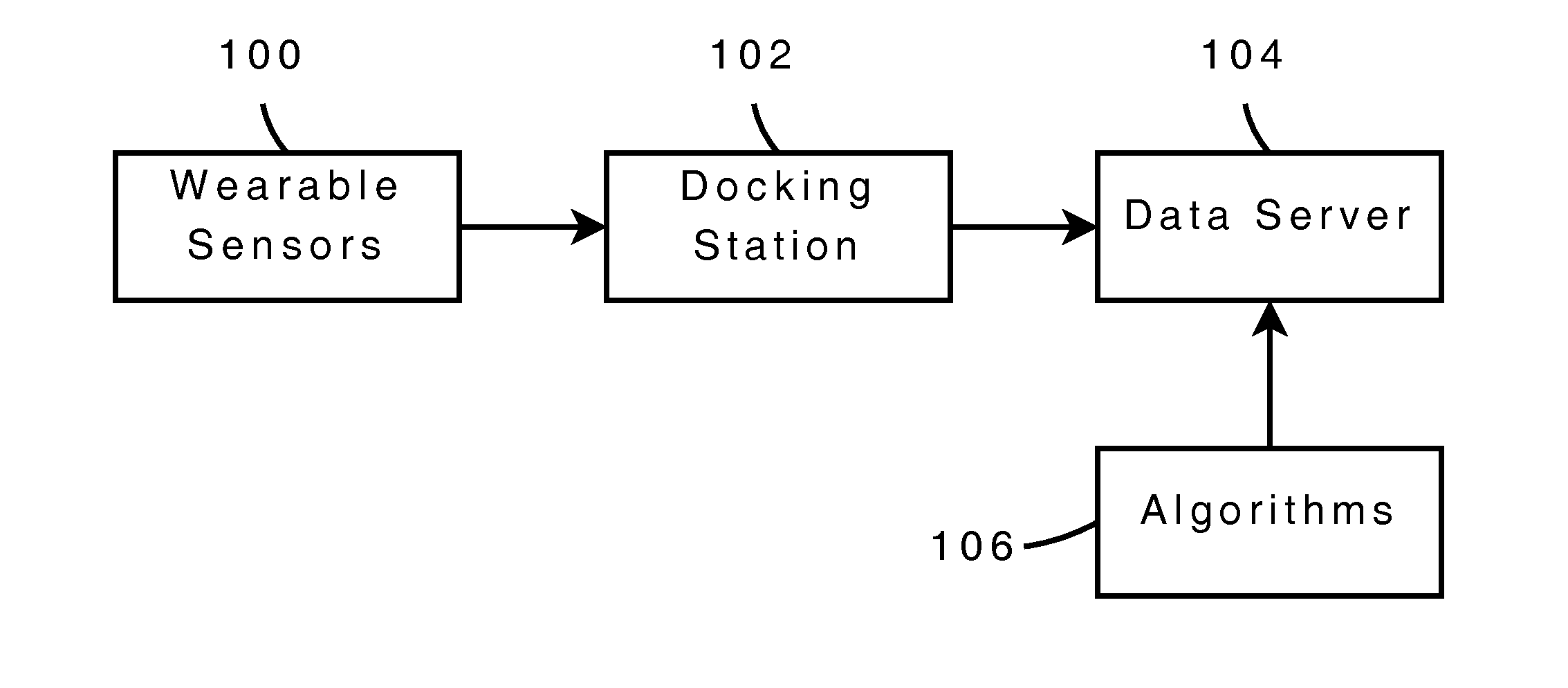
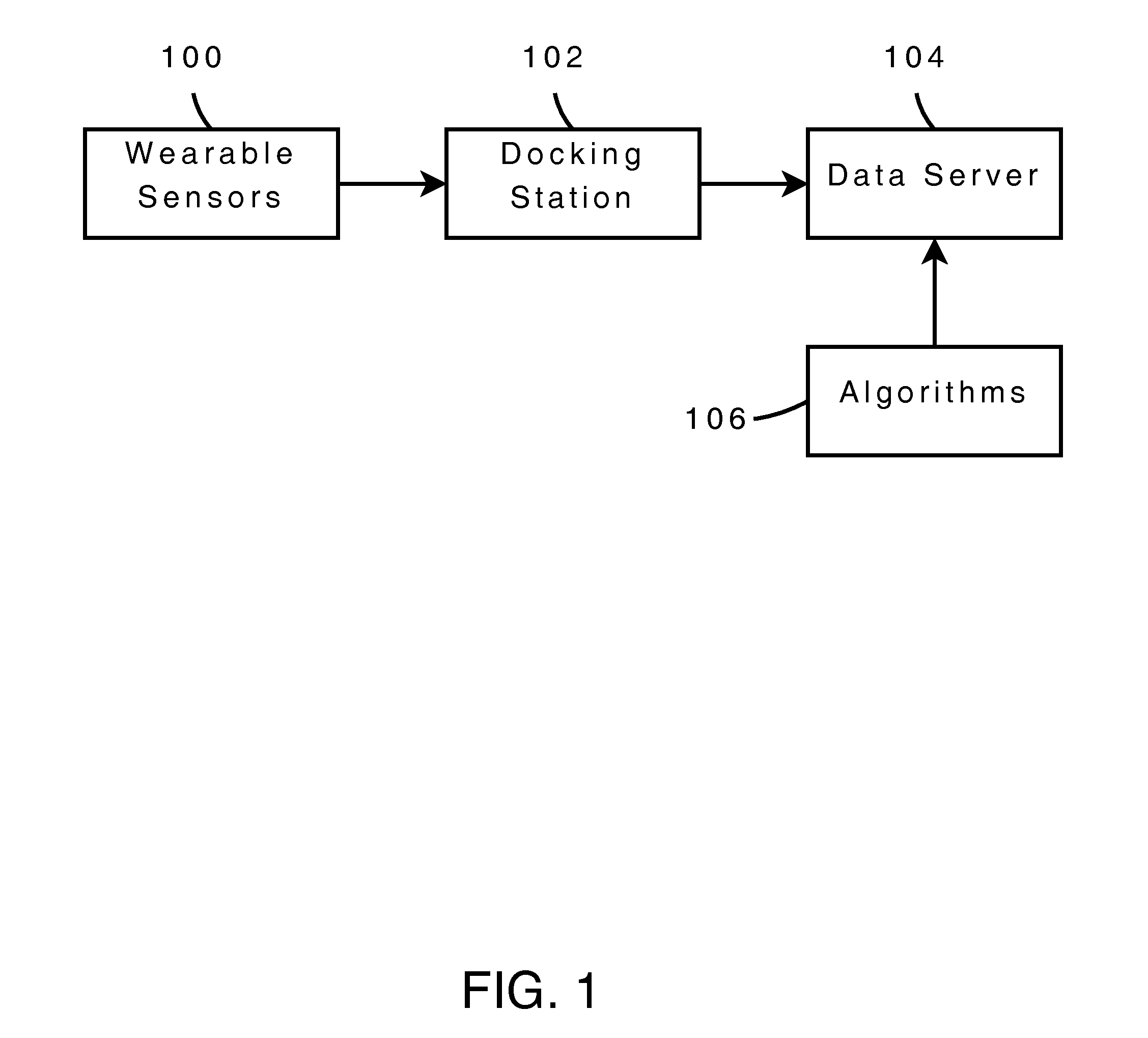
Finally, the limited solutions currently available are device-centric and do not include a complete platform to perform collection, monitoring, uploading, analysis, and reporting.



 Login to View More
Login to View More  Login to View More
Login to View More