

Apparatus for fitting a shoulder prosthesis
a shoulder prosthesis and applicator technology, applied in the field of inverted or anatomical shoulder prosthesis, can solve the problems of prosthesis dislocation and pain of patients, and achieve the effects of reducing interference risk, promoting relative rotation, and increasing tension in the rotator muscles
- Summary
- Abstract
- Description
- Claims
- Application Information
AI Technical Summary
Benefits of technology
Problems solved by technology
Method used
Image

Examples
Embodiment Construction
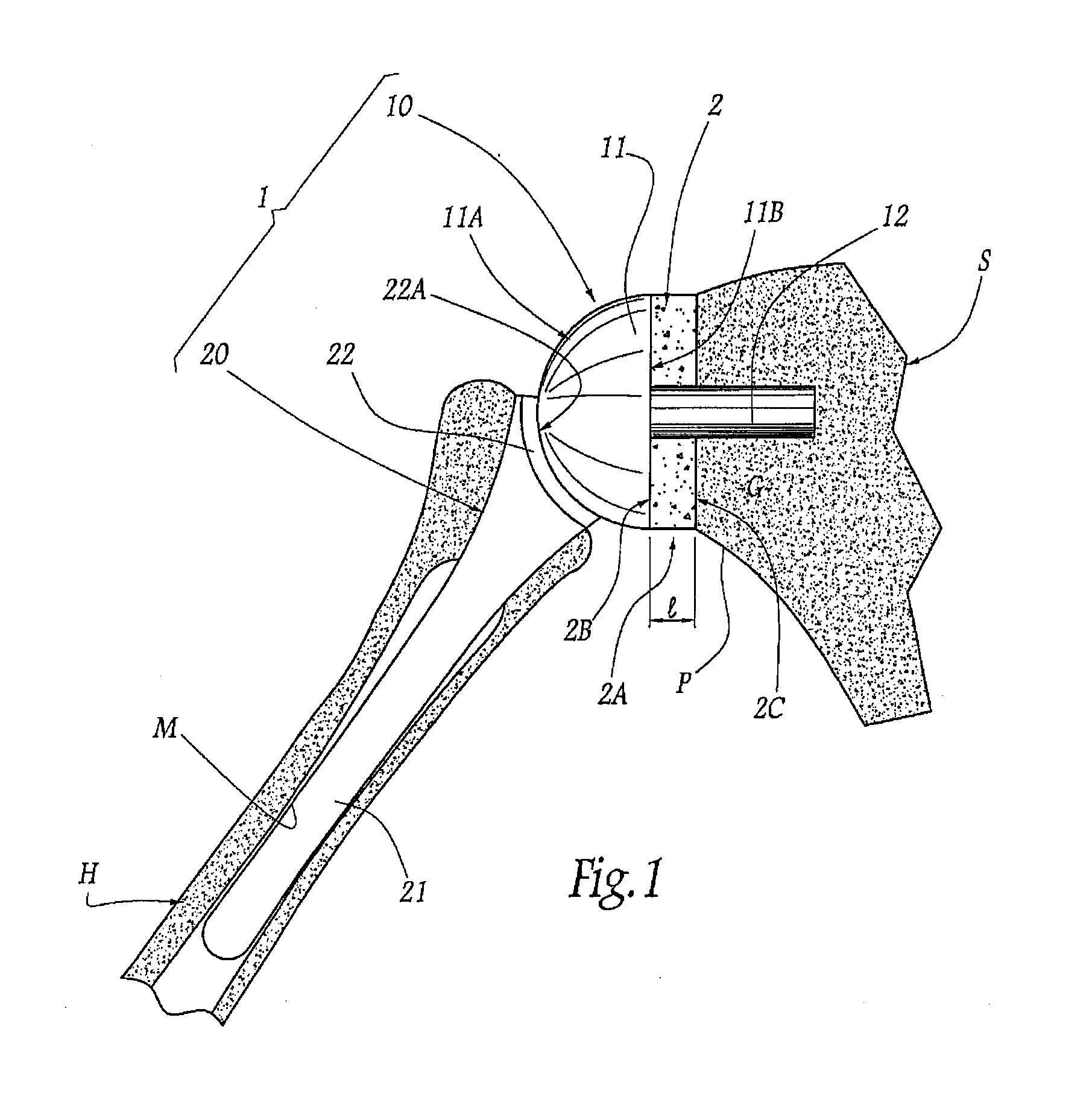
[0047]FIG. 1 shows a shoulder prosthesis 1 comprising a glenoid component 10 and a humeral component 20, respectively implanted in the scapula S and the humerus H of a patient's shoulder. The glenoid components shown herein are illustrated schematically. The method and apparatus of the various embodiments disclosed herein may be used with a variety of other glenoid components, such as for example those disclosed in U.S. Pat. Nos. 7,033,396; 6,953,478; 6,761,740; 6,626,946; 5,702,447 and U.S. Publication Nos. 2004 / 0220673; 2005 / 0278030; 2005 / 0278031; 2005 / 0278032; 2006 / 0020344, which are hereby incorporated by reference.
[0048]The glenoid component 10 comprises a head 11, also described as a head structure, which has, on the side opposing the glenoid surface G of the scapula S, a convex articular surface 11A, also described as a face, of generally hemispherical shape and, on the side turned toward the glenoid surface, an opposing face 11B. In the example considered in the figures, thi...
PUM
| Property | Measurement | Unit |
|---|---|---|
| thick | aaaaa | aaaaa |
| length | aaaaa | aaaaa |
| strength-to-weight ratio | aaaaa | aaaaa |
Abstract
Description
Claims
Application Information
 Login to View More
Login to View More