

Methods and systems for increasing the bending stiffness and constraining the spreading of a spinal segment
a technology of bending stiffness and spinal segment, applied in the field of methods, can solve problems such as limited movement range, and achieve the effects of reducing the risk of injury, and increasing the bending stiffness
- Summary
- Abstract
- Description
- Claims
- Application Information
AI Technical Summary
Benefits of technology
Problems solved by technology
Method used
Image

Examples
Embodiment Construction
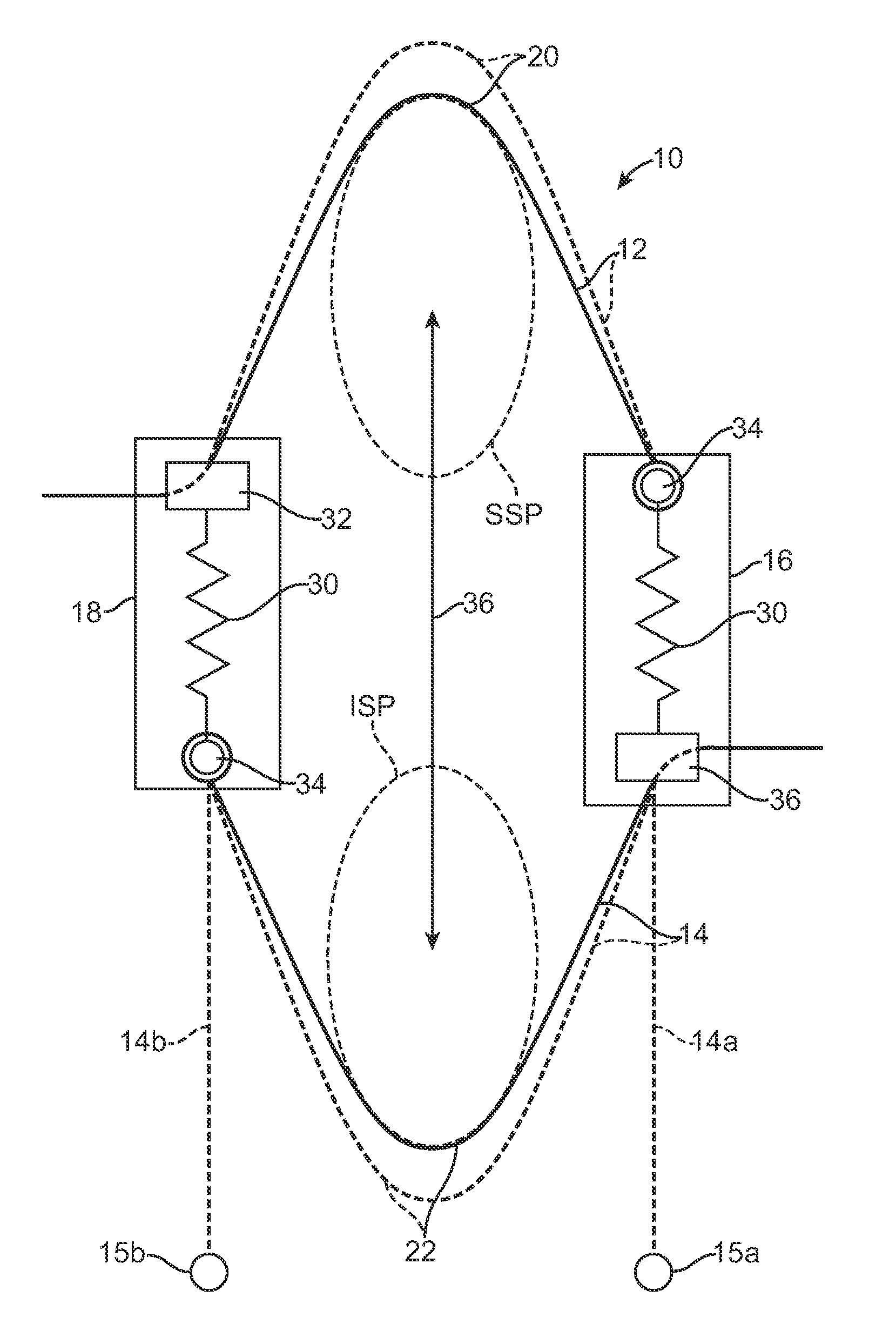
[0061]Exemplary spinous process constraints according to the present invention are illustrated schematically in FIG. 3. The systems 10 comprise a superior tether structure 12, and inferior tether structure 14, and right compliance member 16 and a left compliance member 18. The superior tether structure 12 will typically be a continuous band, cable, strap, cord, or other structure which extends between the two compliance members and provides a saddle region 20 which is adapted to lie over and conform to a superior surface of a superior spinous process SSP as described in more detail in the related prior applications which have been incorporated herein by reference. The inferior tether structure 14 will typically comprise a band, cable, or the like which is constructed similarly if not identically to the superior tether structure 12 and has a saddle region 22 adapted to lie over and conform to an inferior surface of an inferior spinous process 22. In certain instances, however, the in...
PUM
 Login to View More
Login to View More Abstract
Description
Claims
Application Information
 Login to View More
Login to View More