Damage to this nerve compromises both of these functions and arrests the vocal fold just lateral to the midline.
In bilateral
paralysis, there is a loss of abductory function in both folds, the voice may be minimally impaired because of fold symmetry and their paramedian position in most of the patients, but
airway discomfiture is usually severe.
In some situations, however, the condition may be life-threatening.
However, in many cases,
muscle reinnervation is either incomplete or inappropriate resulting in chronic
paralysis.
Although these conventional methods of treatment have been useful, they are less than ideal, since they tend to improve upon one laryngeal function at the expense of another.
However, these procedures compromise voice and
airway protection to restore ventilation through the mouth.
However, a more conservative stance toward resection increases the probability of failed intervention and the necessity for revision
surgery.
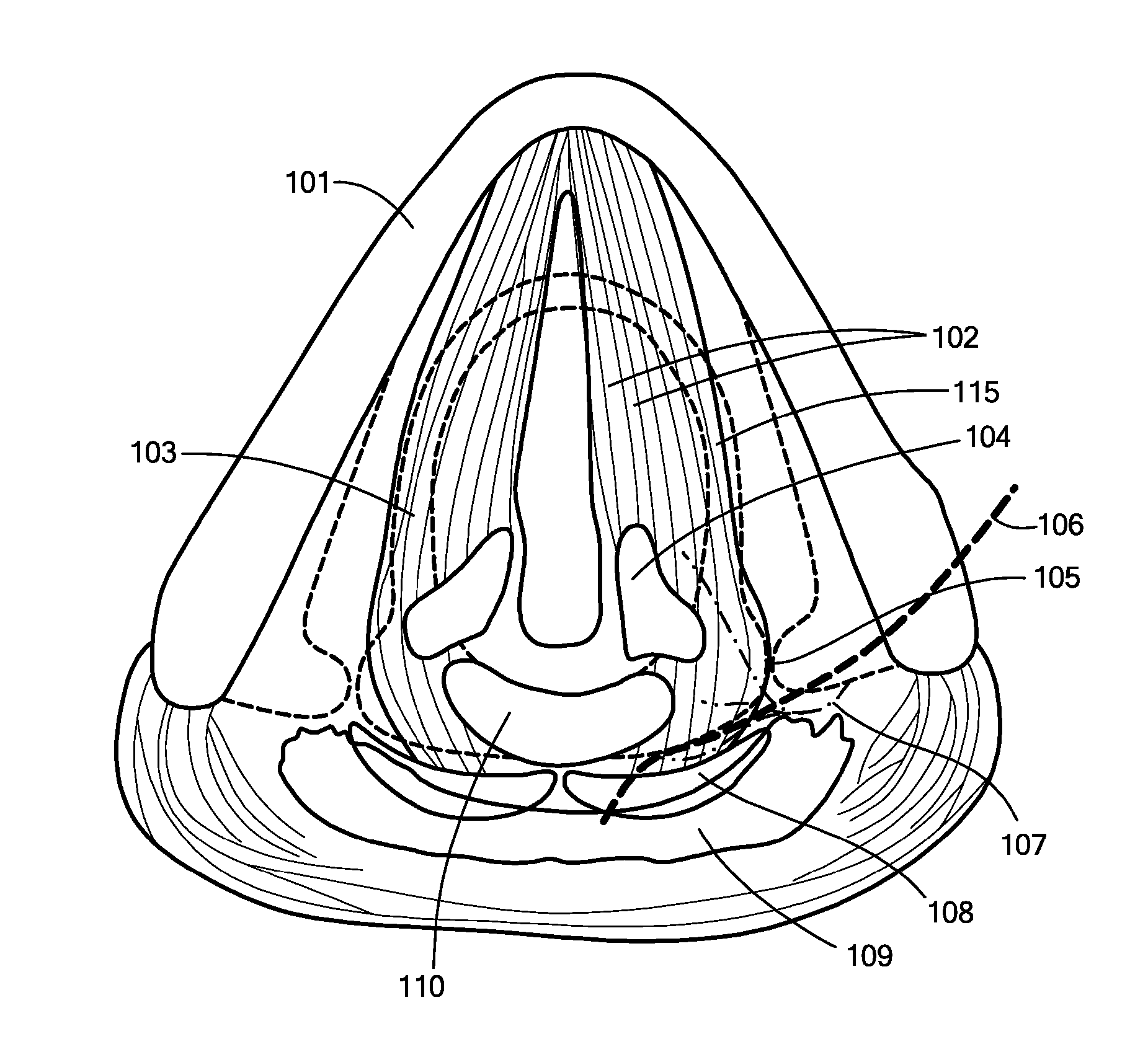
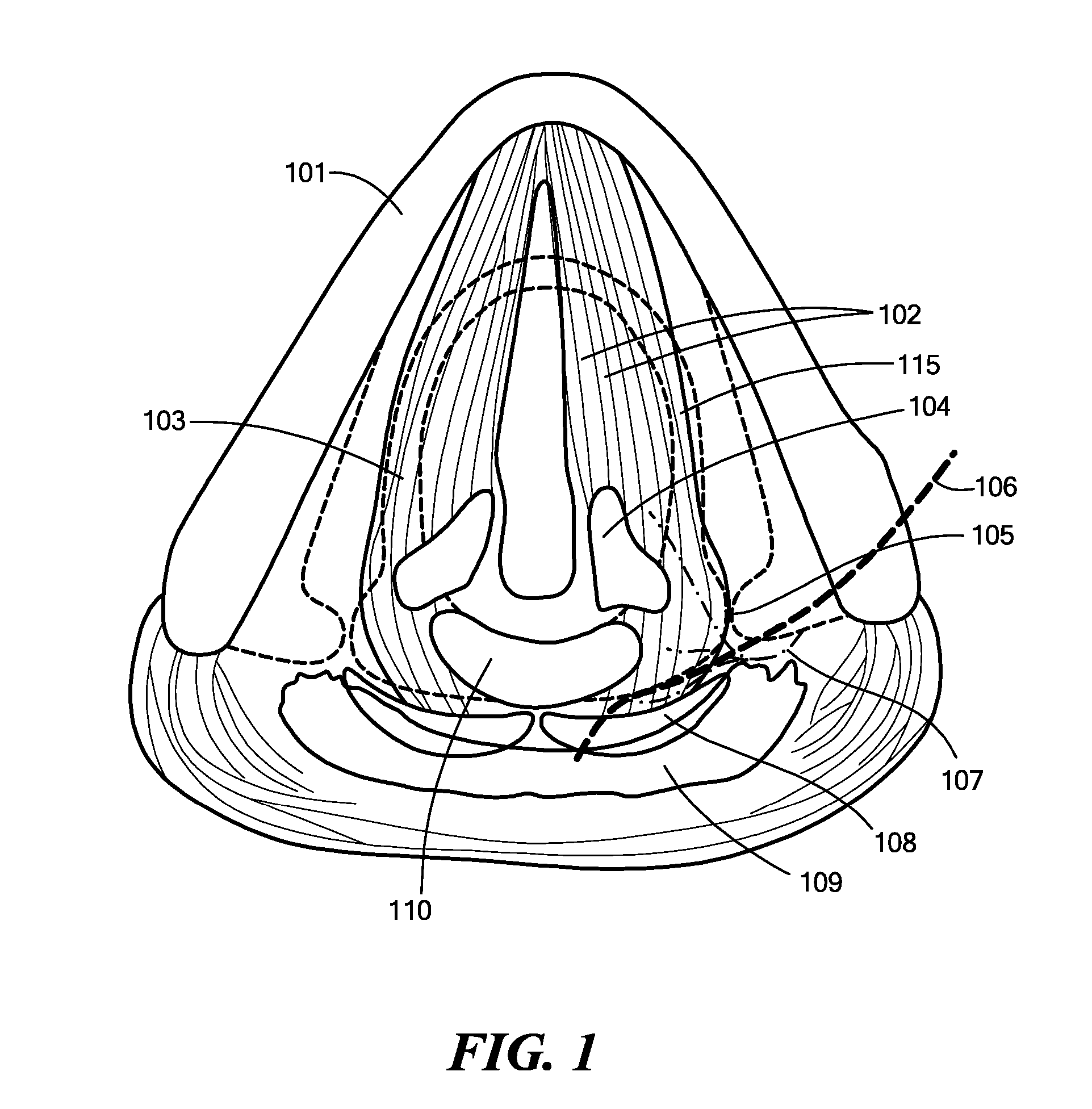
Patients normally breathe well, but they cannot approximate both
vocal folds.
As a result, their voice is weak and breathy, and they tend to aspirate fluids.
As simpler
surgical methods were discovered to restore function in unilateral vocal fold
paralysis, the development of an implantable neuroprostheses for this condition has not been vigorously pursued.
However above 2 ms, stimulation became less efficient for both muscles because of
charge loss through current shunts normally found in tissue.
These recordings showed inappropriate firing patterns.
This may be accomplished by placing the electrodes inside the
muscle, or on its surface, a procedure that produces two technical problems: (1) surgical
exposure of the
muscle causes scarring which eventually decreases muscle mobility; and (2) because electrodes must be close to their target to be efficient, they are exposed to
muscle movement.
This difficulty plagued the early development of the cardiac pacer and persists today in many experiments involving chronic stimulation of denervated muscle, including the denervated PCA.
As a result, there has not been a truly successful chronic device for stimulation of denervated muscle.
This method is not applicable for the clinically more relevant bilateral paralysis.
For a real and complete
rehabilitation of some patients with uni- or bilateral vocal cord paralysis or even in patients with a
larynx transplantation a mere restoration of a single movement function of vocal cords by a pacemaker is not sufficient.
Furthermore, scarring of all those tissues may diminish stimulated movements in the long run.
In addition, free placement of electrodes through the tissue to the target muscle (or nerve) may cause a high mechanical stress in the
electrode leads which may cause lead
wire breakage in delicate electrodes.
This may be accomplished by placing the electrodes inside the muscle or at its surface, a procedure that produces two technical problems: (1) surgical
exposure of the muscle causes scarring which eventually decreases the muscle's mobility; and (2) because electrodes must be close to their target to be efficient, they are exposed to
muscle movement.
The constant abrasion of the electrode against muscle breaks the electrode or causes extensive
fibrosis in the muscle.
This difficulty plagued the early development of the cardiac pacer and persists today in many experiments involving chronic stimulation of denervated muscle, including the denervated PCA.
As a result, there is not currently a truly successful chronic device for stimulation of denervated muscle.
For some situations, however, it is not possible to reach the target point (e.g., inside the subject's body or a different position outside the body then where the
insertion started) in a straight line from the outside of the body or starting from cavities inside the body.



 Login to View More
Login to View More  Login to View More
Login to View More