[0009] In a first embodiment, a method of forming a transmural
lesion in a wall of the heart adjacent to the pulmonary veins comprises the steps of placing at least one ablation device through a thoracic incision and through a pericardial penetration so that at least one ablation device is disposed in contact with an epicardial surface of the
heart wall; positioning at least one ablation device adjacent to the pulmonary veins on a posterior aspect of the heart while leaving the pericardial reflections intact; and ablating the
heart wall with at least one ablating device to create at least one transmural
lesion adjacent to the pulmonary veins. While the method may be performed with the heart stopped and circulation supported with
cardiopulmonary bypass, the method is preferably performed with the heart beating so as to minimize morbidity, mortality, complexity and cost.
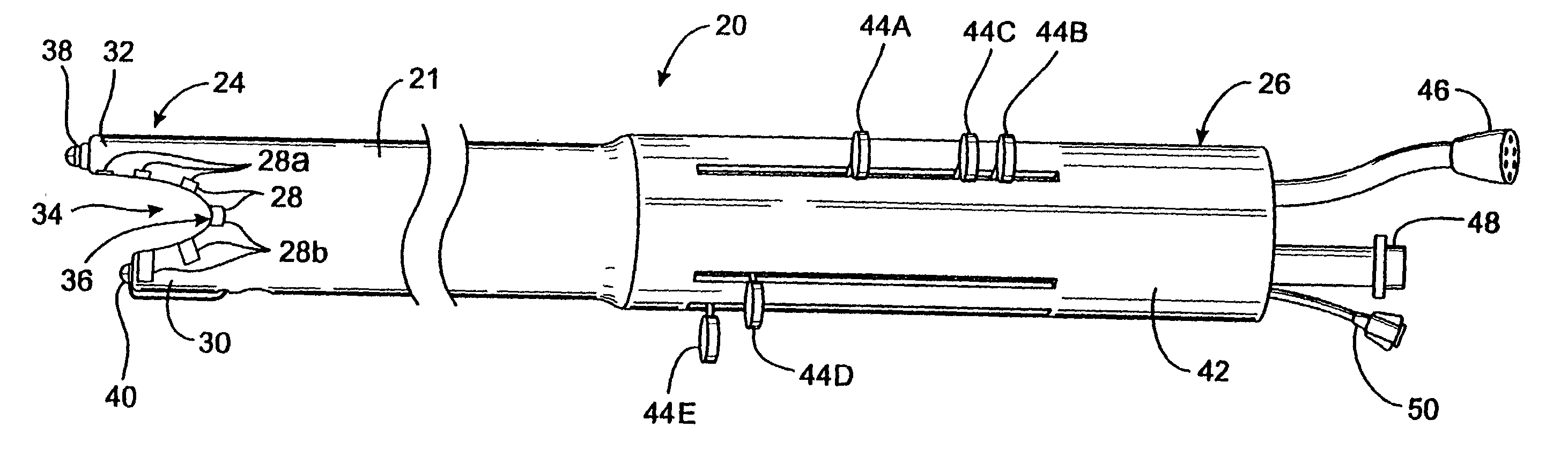
[0012] In addition, a mechanism may be provided for urging all or part of the working end against the epicardium to ensure adequate contact with the ablation devices. This mechanism may be, for example, one or more suction holes in the working end through which suction may be applied to draw the working end against the epicardium, or an
inflatable balloon mounted to the outer side of the working end such that, upon inflation, the
balloon engages the inner wall of the
pericardium and forces the working end against the epicardium. This also functions to protect extracardiac tissues such as the
pericardium from injury by retracting such tissues away from the epicardial region which is being ablated, and, in the case of the
balloon, providing an insulated barrier between the electrodes of the ablation probe and the extracardiac tissues.
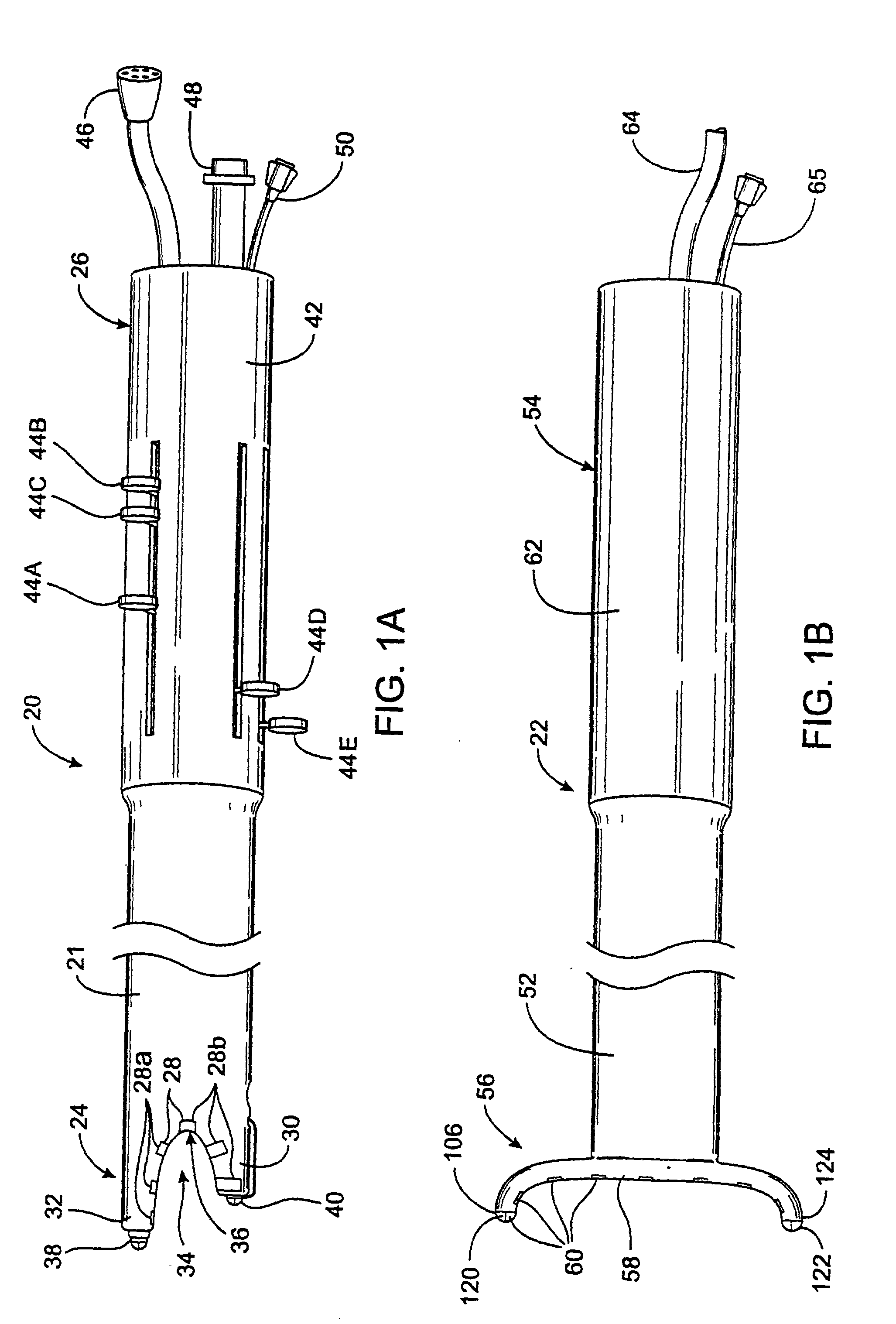
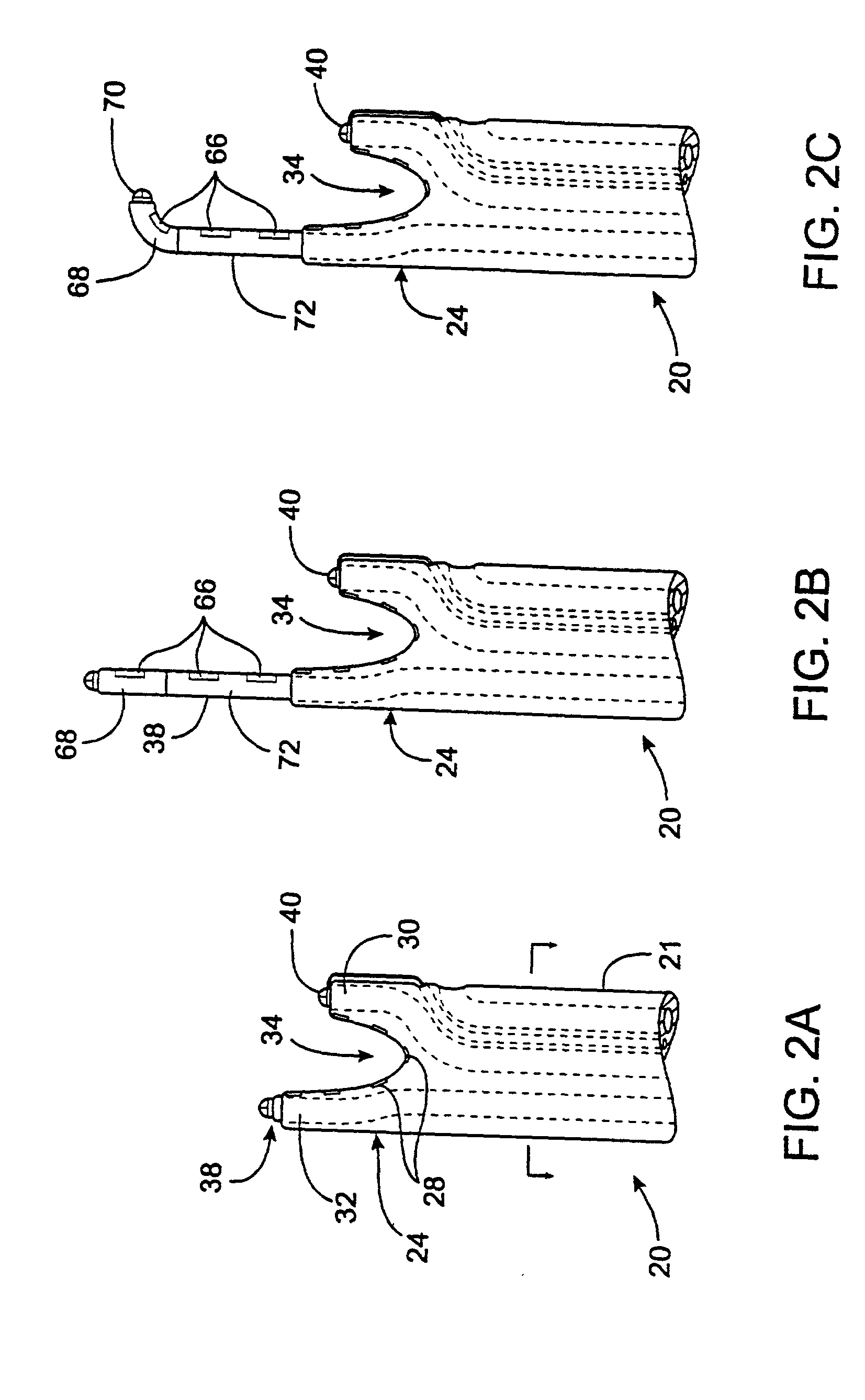
[0013] The apparatus may be either a single integrated device or two or more devices which work in tandem. In either case, the apparatus may have two or more tips at the working end which are positioned on opposing sides of a tissue layer such as a pericardial reflection. A device may be provided for approximating the two free ends on opposing sides of the tissue layer, such as an
electromagnet mounted to one or both of the free ends. In this way, a continuous
lesion may be created in the myocardium from one side of the pericardial reflection to the other without
puncturing or
cutting away the pericardial reflection.
[0023] The device also has a fluid inlet and a fluid outlet for delivering and withdrawing fluid from within the closed wall formed by the inner lip. The fluid is preferably a
conductive fluid, such as hypertonic
saline, which conducts energy from the ablating element, such as an RF
electrode, to the tissue. The fluid is preferably delivered along a
short axis of the ablating element so that the temperature change across the ablating element is minimized.
[0026] In a further aspect of the invention, the ablating element preferably produces
focused ultrasound in at least one dimension. An
advantage of using
focused ultrasound is that the energy can be concentrated within the tissue. Another
advantage of using focused
ultrasound is that the energy diverges after reaching the focus thereby reducing the possibility of damaging tissue beyond the
target tissue as compared to collimated ultrasonic energy. When ablating epicardial tissue with collimated
ultrasound, the collimated
ultrasound energy not absorbed by the
target tissue travels through blood and remains concentrated on a relatively small area when it reaches another surface such as the endocardial surface on the other side of a
heart chamber. The present invention reduces the likelihood of damage to other structures since the ultrasonic energy diverges beyond the focus and is spread over a larger area. The focused ultrasound has a
focal length of about 2 to 20 mm, more preferably about 2 to 12 mm and most preferably about 8 mm in at least one dimension. The focused ultrasound also forms an angle of 10 to 170 degrees, more preferably 30 to 90 degrees and most preferably about 60 degrees as defined relative to a focal axis. The focused ultrasound preferably emits over 90%, and more preferably over 99%, of the energy within the angles and focal lengths described above. The focused ultrasound may be produced in any manner and is preferably produced by a curved
transducer with a curved layer attached thereto. The ultrasound is preferably not focused, and may even diverge, when viewed along an axis transverse to the focal axis.
[0032] The device may be adhered to tissue with suction although suction is not required. The device may also have a membrane filled with a substance which transmits the
ultrasound energy to the tissue. The membrane conforms to the tissue and eliminates air gaps between the device and tissue to be ablated. Alternatively, the device may have a
solid element which contacts the tissue and transmits the
ultrasound energy to the tissue. The device may also be used with a gel applied to the tissue which transmits the
ultrasound energy and eliminates air gaps.



 Login to View More
Login to View More  Login to View More
Login to View More