Unfortunately, sophisticated MV delivery systems may not be able to treat superficial cancers such as those of the
skin or nonmalignant lesions of the
skin such as keloids.
This inability to treat superficial lesions is due to the nature of the differential dose deposited at depth with MV energy x-rays; these x-rays deliver a much lower dose within mm to cm of the surface than they do at depth due to the buildup of dose from scattered electrons as the beam passes through tissue.
Thus it is difficult to deliver enough dose near the
skin surface without overdosing tissue
lying under the skin.
MV delivery systems also may not be applicable for use in the treatment of tumors that receive
radiation therapy at the time of
surgery.
However, conventional MV radiation equipment is very heavy and large and requires thick concrete walls to contain the
stray radiation produced by the equipment.
This has restricted OR-based IORT to a handful of hospitals that have been able to absorb the high costs associated with the equipment and the construction of large shielded room in the OR.
This method of IORT involves very complex logistics, increases
patient risk, severely limits the number of patients that can be treated, and reduces the potential
efficacy of the treatment.
MV devices have a range of other problems as well.
Ranging in price from $1 M to in excess of $4 M depending on features, external beam megavoltage delivery devices are very complicated to build and are quite
time consuming when it comes to creating a plan for delivering the treatment and in actually delivering the treatment.
They require constant and expensive maintenance and monitoring, suffer from significant
downtime, and only can be used by highly trained personnel working in dedicated departments.
Their major disadvantages are that they are not as easy to characterize and plan for as are photons and they add cost to the price of the already expensive MV device (which is used to generate them).
They also have limitations when used to treat lesions that are directly under the
skin surface.
In terms of IORT, although much more mobile and
user friendly than their predecessors, mobile
electron units still weigh close to one
ton and are large and ungainly, making it difficult to move them around in an OR and bring them in opposition to the treatment site, and are expensive in terms of user and patient time.
They also are relatively imprecise in terms of their ability to treat irregularly shaped tumors and are quite time-consuming to plan for and use.
The major downside to low energy x-rays that has limited severely their use in modern day
cancer treatment is that they have very poor penetration in tissue.
They have also a surface dose that is as much as a hundred times more than the dose at depth resulting in the potential for severe skin reactions when treating deeper lesions.
As a result therapeutic low energy x-rays delivered by traditionally means are very limited in their applications.
This approach has been explored for use in radiosurgical treatments but is severely limited for superficial applications.
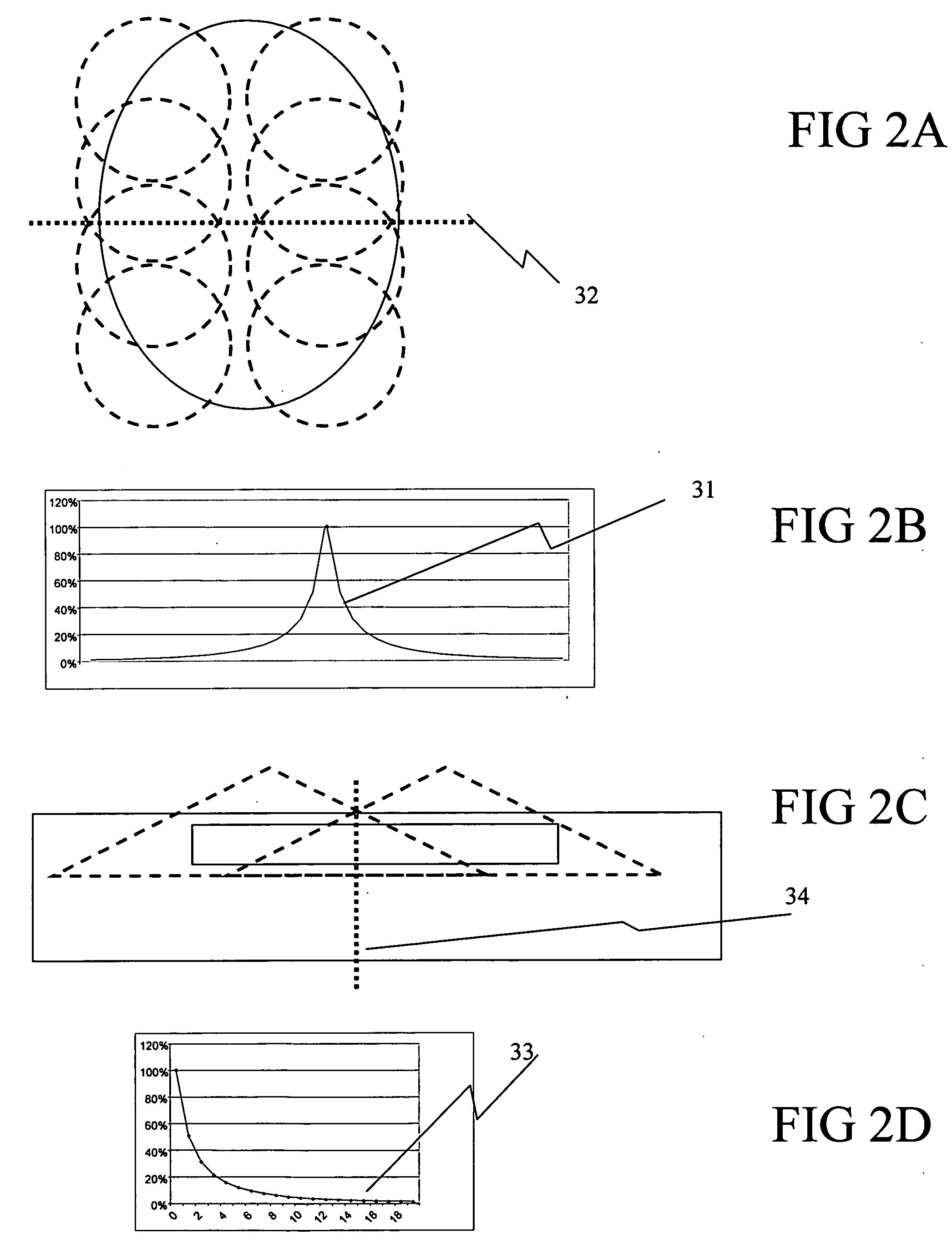
Unfortunately, because the
depth of penetration of KV x-rays is so poor, there are limited geometries that can be used through which to rotate the beam for superficial target locations, resulting in only several degrees of rotation and therefore very little increase in dose at depth or lowering of skin dose.
Although such can be designed as an add-on device to an existing orthovoltage systems, it increases the cost very significantly and prices it out of the reach of practicing physicians.
It also is quite inefficient, as the reduction in skin dose and the increase in treatment depth and
dose rate at depth are achieved by concentrating the x-
ray beam at a very small spot, the gains being proportional to the decrease in spot size.
Thus larger lesions would need to be treated by scanning the spot across the target, achieved either by moving the patient under the delivery device or by mounting the delivery device in such a manner that the spot can be scanned over an immobilized patient; either approach adds considerably to the cost of the overall
system.
In addition, it is not meant to treat superficial lesions; the process of focusing the dose would result in a potential increase in skin dose if the treatment were delivered to a superficial location.
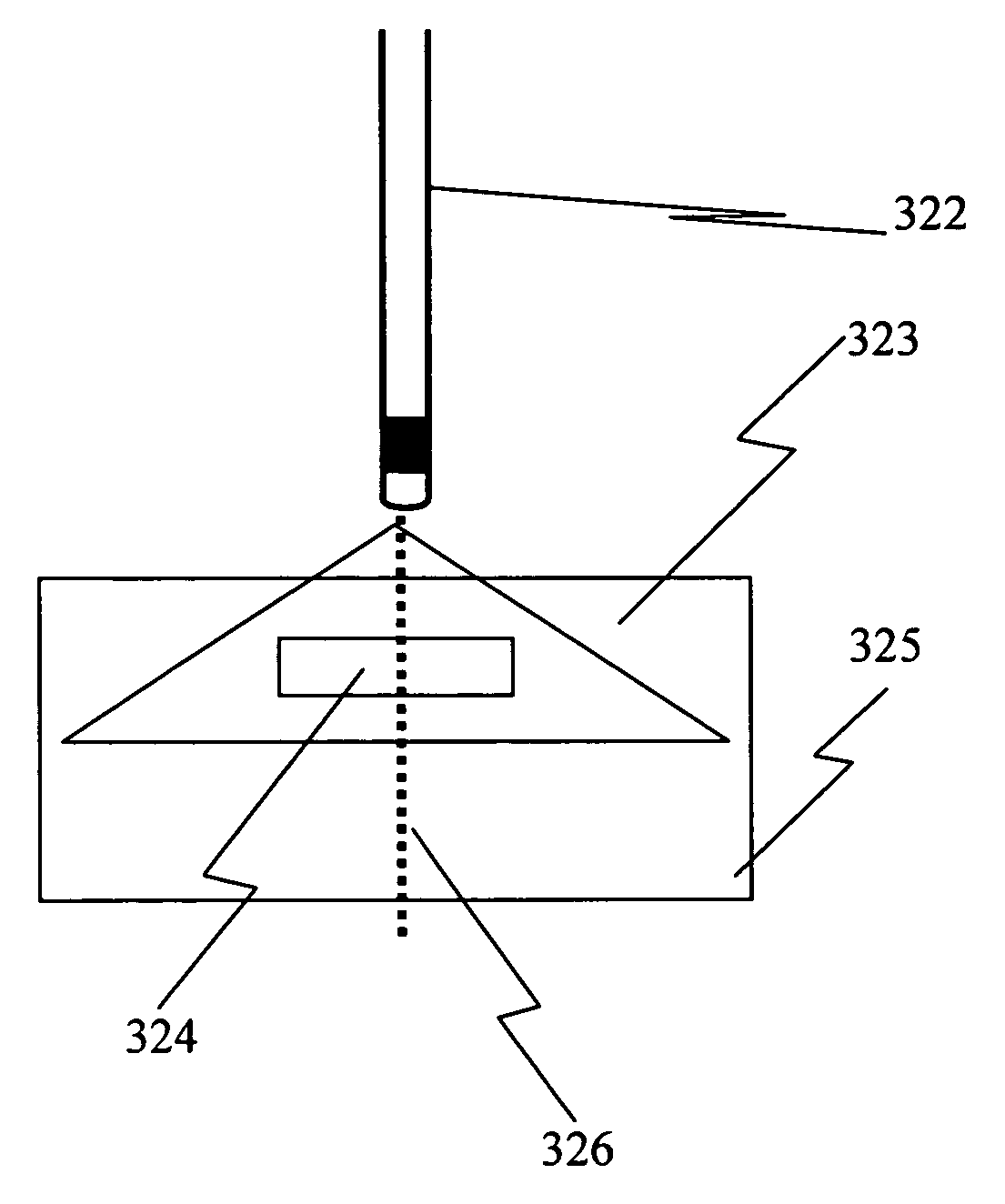
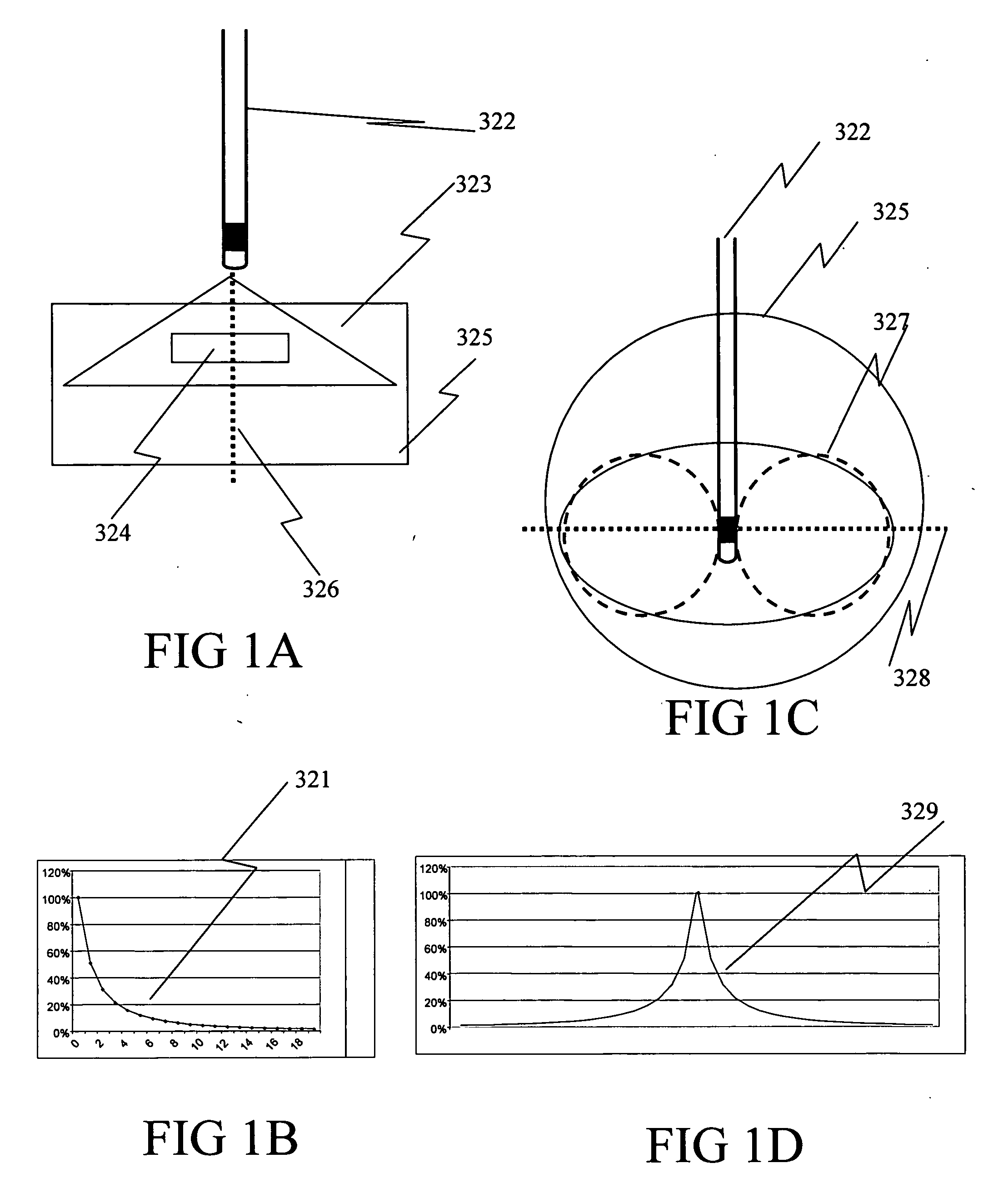
This approach also is plagued by the problems inherent to date in using low energy x-rays, namely the dose where the x-
ray beam first enters tissue at the center of the volume being treated is very much greater than the dose in the rest of volume being treated.
Attempts have been made to mitigate this problem by using multiple electronic x-
ray sources or multiple positions of a single x-ray source but this increase the invasiveness of the procedure.
However, the problem with radioactive isotopes is the same as with KV or low energy radiation—the dose is very much higher at the point(s) where the dose enters the tissue than at any other place.
This makes it very difficult to deliver a uniform dose to a thickness of tissue or to deliver a dose at depth that is greater than the dose delivered to the
tissue surface.
There also are problems associated with defining the region to be treated and to making sure that the correct region is treated.
This is a process that, because of its complexity and the difficulty in positioning patients, is prone to error.
This is only theoretical because all known therapies have side effects that limit their usefulness.
However, because this single dose of radiation also will kill all surrounding and interwoven normal cells within the
treatment field, it is limited currently in the types of tumors it can treat.
Also, its cost, believed to cost in excess of $5 M for equipment, room, and specialized supporting infrastructure, limits its availability.
Unfortunately, the marginal difference between the effect of radiation on
malignant cells and normal cells is not great enough to allow radiation to be delivered to both regions indiscriminately, even with
fractionation without incurring serious side effects.
As a result much time and effort has gone into designing equipment and creating delivery techniques that allow the greatest possible
physical separation between normal and
malignant cells so that the normal cells will receive less radiation than the
malignant cells.
However, modern day
radiation therapy may have reached its limit in terms of its ability to eliminate or control cancer, especially for invasive cancers where the malignant cells intermix with normal cells such that killing the former also will kill the latter.
IGRT reduces the amount of
normal tissue that is included in the treatment volume but cannot eliminate it entirely.
Although metabolic imaging techniques can provide additional information about cancer location, the designation of a target volume is still a physician-based process, fraught with inter- and intra-user variability and with an inability to differentiate
disease from normal at the
cellular level.
In addition, many cancers contain radioresistant regions in their center due to poor
oxygenation.
However, the amount of radiation required to kill the initial group of oxygenated cells uses up all of the
normal tissue reserve; the interior cells once oxygenated cannot be treated with additional radiation without destroying surround
normal tissue.
The limited
efficacy and extended
toxicity of traditional
single agent cytotoxic therapy such as radiation therapy has led researchers to explore the design and development of targeted binary therapies that differentiate between, and thereby augment the effect on, malignant cells as compared to nonmalignant cells.
The
disadvantage of this approach is that the process for generating the
Auger electrons must take place within the
cell.
As a result, such a therapy has the potential for repetitive dosing with minimal
toxicity.
However, these agents do not identify cancer cells directly.
In addition, it is often difficult to deliver enough contrast agent to the region in question by the IV
route in order to achieve significant enough dose enhancement.
Direct injection allows for a higher concentration of contrast agent, but it requires an
invasive procedure that may not
gain access to all tumors.
The major downside to low energy x-rays that limits their use in dose enhancement applications is their very poor penetration in tissue as described previously.
However, even using 10 fields will only result in a dose at depth that is at best equal to 10% of the dose at the skin.
Unfortunately, the same problems discussed preciously that apply to each of the low energy x-ray delivery approaches without the use of dose enhancement apply to their use with dose enhancement, namely a high cost, complexity, a lack of portability, lengthy treatment times, and limited available geometries restricting applicability, apply when used with dose enhancement.
Unfortunately, this is a $100 million device based on a
cyclotron that limits severely its availability and suitability.



 Login to View More
Login to View More  Login to View More
Login to View More