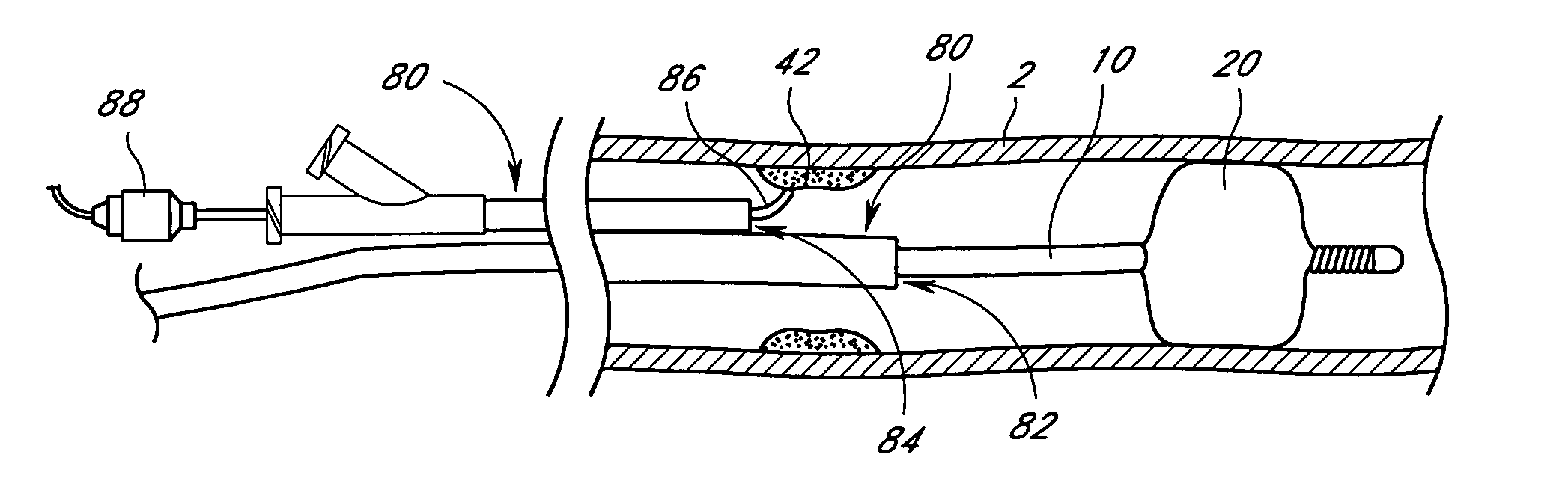
As can be readily appreciated, the withdrawal of treatment catheters over a placed guidewire may result in the guidewire being displaced from its position.
Cohen also does not address the problem of emboli containment.
However, many blood vessels where it is desirable to apply catheter treatment are quite narrow.
Similarly, saphenous
vein grafts (SVG) and the
carotid arteries are also quite small and susceptible to plaque, and could not practically be treated by larger
diameter devices.
Human blood vessels often become occluded or completely blocked by plaque, thrombi, other deposits, emboli or other substances, which reduce the blood
carrying capacity of the vessel.
Should the blockage occur at a critical place in the
circulatory system, serious and permanent injury, or even death, can occur.
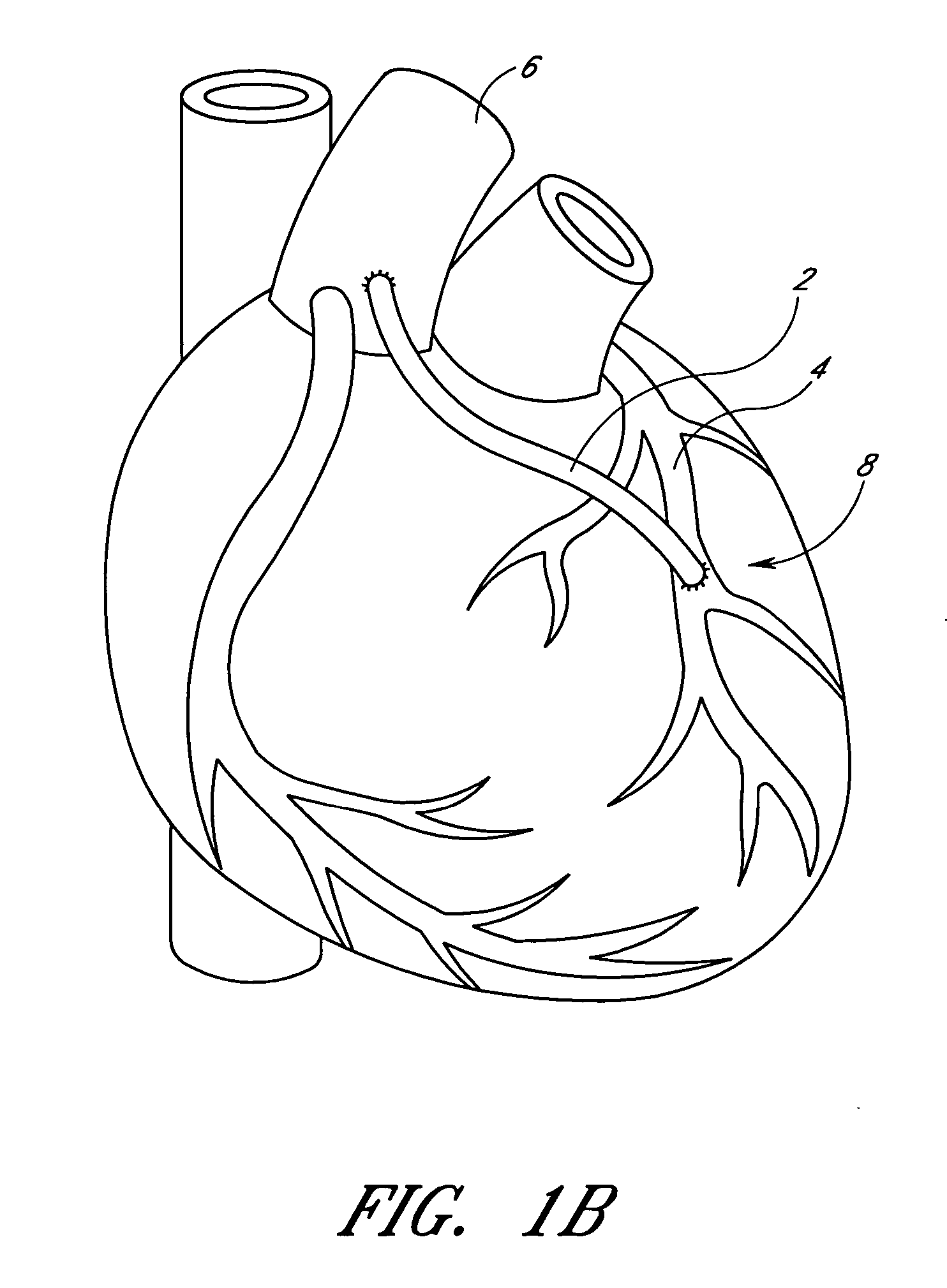
The
coronary arteries are first narrowed and may eventually be completely blocked by plaque, and may further be complicated by the formation of thrombi (blood clots) on the roughened surfaces of the plaques.
Myocardial infarction can result from atherosclerosis, especially from an occlusive or near occlusive thrombi overlying or adjacent to the atherosclerotic plaque, leading to death of portions of the heart
muscle.
It can be difficult, however, to treat plaque deposits and thrombi in the coronary arteries, because the coronary arteries are small, which makes accessing them with commonly used catheters difficult.
Each of these methods are not without the risk of
embolism caused by the dislodgement of the blocking material which then moves downstream.
In addition, the size of the blocked vessel may limit
percutaneous access to the vessel.
In coronary
bypass surgery, a more costly and invasive form of intervention, a section of a vein, usually the saphenous vein taken from the leg, is used to form a connection between the
aorta and the coronary
artery distal to the obstruction.
Over time, however, the saphenous
vein graft may itself become diseased, stenosed, or occluded, similar to the bypassed vessel.
Once the plaque and thrombi are dislodged from the vein, they can move downstream, completely blocking another portion of the coronary artery and causing
myocardial infarction.
Therefore,
balloon angioplasty of vein grafts is performed with the realization that involvement by friable atherosclerosis is likely and that atheroembolization represents a
significant risk.
Because of these complications and high recurrence rates, old diffusely diseased saphenous vein grafts have been considered contraindications for
angioplasty and
atherectomy, severely limiting the options for minimally invasive treatment.
However, such arteries have been very difficult to treat because of the possibility of dislodging plaque which can enter various arterial vessels of the brain and cause permanent
brain damage.
Attempts to treat such occlusions with
balloon angioplasty have been very limited because of such dangers.
Such
surgical procedures have substantial risk associated with them which can lead to morbidity and mortality.
In other procedures, such as in angioplasty and in the treatment of
peripheral arteries and veins, there is the possibility that the
guide wires and catheters used in such procedures during deployment of the same may cause dislodgement of debris or emboli which can flow downstream and cause serious damage, such as
stroke, if they occlude
blood flow in smaller vessels.
Moreover, when treating aneurysms, coils or other objects deployed to fill the
aneurysm may break free and become lost downstream.



 Login to View More
Login to View More  Login to View More
Login to View More